





Abstract
Facial artery aneurysms are extremely rare. To date, only nine cases have been reported in the literature. We report here the first case in Sub-Saharan Africa, in a 48-year-old male with no significant medical history, who presented with a swelling in the right submandibular region. Following radiological investigations, he underwent successful surgical resection. No complications or recurrence of the aneurysm were noted during a five-year follow-up.
Introduction
Aneurysms of the extracranial vessels of the head and neck are rare and most commonly involve the superficial temporal artery and the facial artery [1]. The most common extracranial vascular lesions are usually false aneurysms secondary to trauma [2]. Facial artery aneurysms are rare, with only nine cases reported in the literature to date [1–9]. In this article, we describe a rare case of a facial artery aneurysm treated with complete surgical resection. To our knowledge, this is the first case to be published in sub-Saharan Africa.
Case report
A 48-year-old man presented with a painful swelling in the right submandibular region that had developed 3 months earlier. He had no known history of cardiovascular disease, smoking, diabetes, or craniocervical trauma. On palpation, the mass was pulsatile and measured ~4 × 3 cm in diameter. Intraoral examination revealed no abnormalities.
Doppler ultrasound of the mass revealed a 19 mm ovoid formation in the right hemi-mandibular region, with arterial waveforms and likely afferent and efferent arteries. Craniocervical computed tomography (CT) (Fig. 1a–c) confirmed a saccular aneurysm of the right facial artery, measuring 23.9 × 17 mm, thrombosed in two-thirds of its lumen.
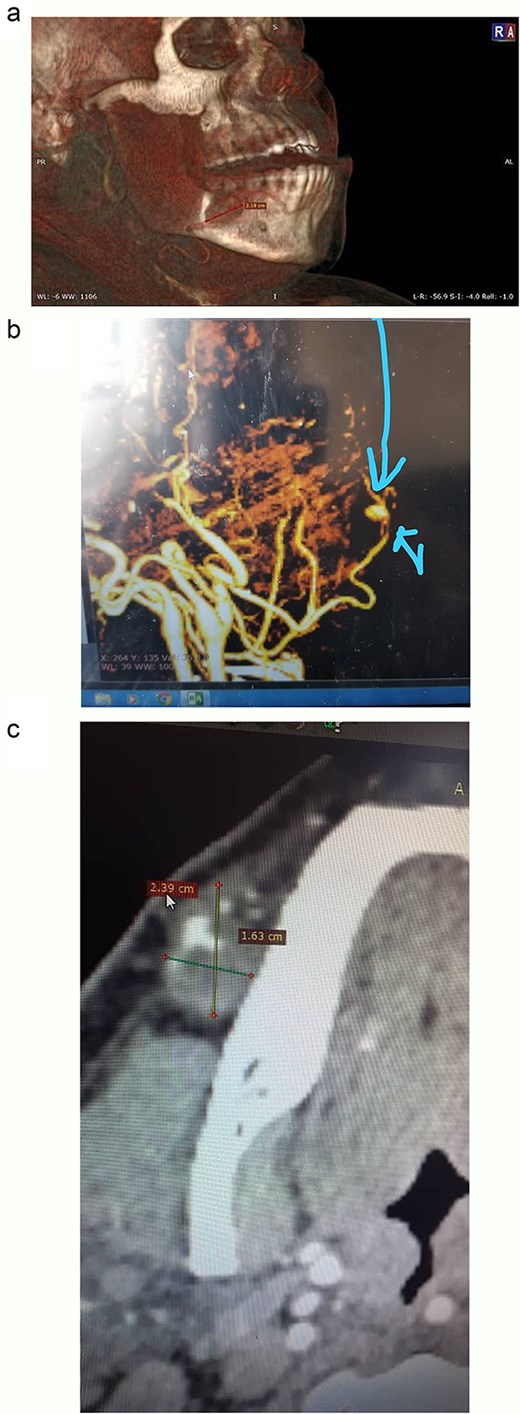
CT images illustrating the right facial artery aneurysm: (a) 3D-reconstructed CT scan highlighting the aneurysm. (b) Preoperative contrast-enhanced CT with 3D reconstruction indicating the aneurysm. (c) Preoperative axial contrast-enhanced CT demonstrating the saccular aneurysm of the right facial artery and its measurements.
He underwent surgical resection under general anesthesia. The aneurysm was located anterior to the masseter muscle, in the posterior and superior regions of the submandibular gland. It was successfully resected without intraoperative complications (Fig. 2). It measured 3 × 3.5 cm in diameter, and its lumen was partially filled with thrombus (Fig. 3).
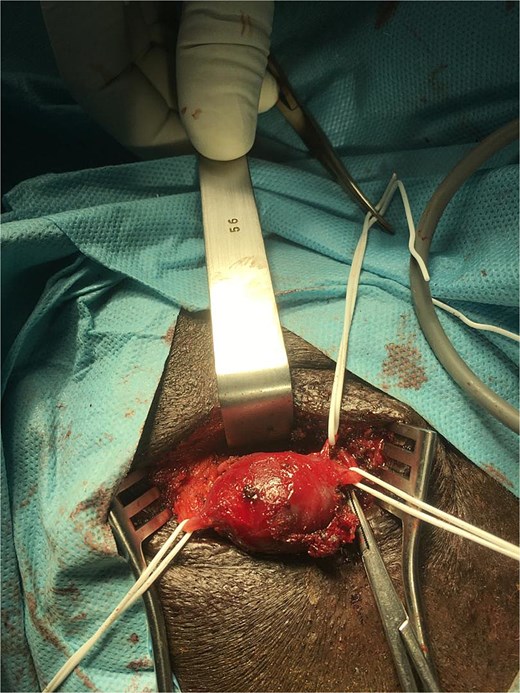
Intraoperative view of the right facial artery aneurysm and its multiple collaterals.
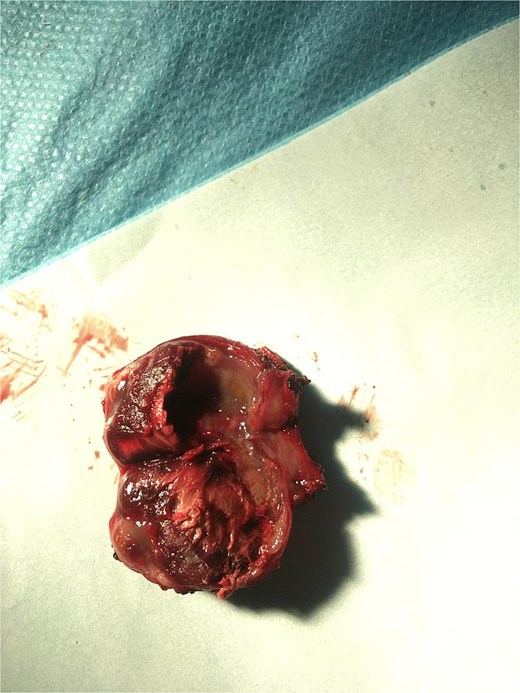
Cross-section of the removed aneurysm.
Histopathological examination revealed an aneurysmal arterial wall showing thrombotic changes with incipient fibrous organization (Fig. 4). After a clinical follow-up of 5 years, no recurrence of the aneurysm was detected.
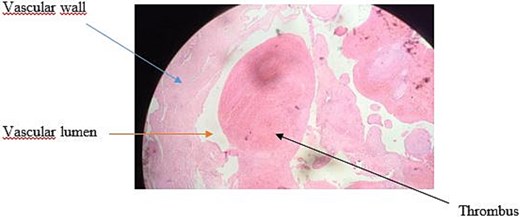
Histological image at intermediate magnification (×10).
Discussion
Facial artery aneurysms are extremely rare, with nine cases reported in the literature to date [1–9]. There is an almost equal distribution between men and women, with four women and five men [1–9]. The age of our patient (48 years) is lower than those reported in the literature, which range from 54 to 79 years [1–9].
Aetiologically, aneurysms can be linked to infections (fungal or syphilitic), congenital anomalies, or atherosclerosis [1]. In several reported cases, hypertension was the most common risk factor [1, 2, 6, 9]. However, four cases, like our patient, had no known comorbidities [3, 5, 7, 8].
Diagnosis of facial artery aneurysms is based primarily on imaging, in particular Doppler ultrasound, and CT angiography [1, 5]. Therapeutic management remains poorly described [4]. Surgical resection, ligation, and embolization are the main options. However, surgical resection may be associated with a risk of hemorrhage and facial nerve injury, whereas embolization may result in recanalization, leading to recurrence [9].
Of the previously reported cases, five patients underwent surgical resection alone [1, 3–6]. Two patients underwent endovascular treatment because of the large aneurysm size and the high risk of facial nerve injury with surgical resection, which is more indicated in patients at high operative risk, particularly for hemorrhage in elderly subjects [2, 8]. One patient underwent surgical resection preceded by internal trapping to prevent intraoperative bleeding [7]. One patient underwent secondary surgical resection after failed embolization [9].
In our sub-Saharan context, surgical resection proved to be a reliable and safe treatment for facial artery aneurysms, with no complications or recurrences at 5 years’ follow-up. This experience highlights the importance of individualized evaluation and adequate surgical resources for the management of arterial aneurysms in Africa.
Conclusion
Facial artery aneurysms are very rare. Diagnosis is based on clinical examination and radiological investigations (Doppler ultrasound and CT angiography). Surgical resection remains a reliable treatment option, offering good outcomes when conditions permit. However, the management of facial artery aneurysms must be individualized, considering the risks and benefits of surgical resection, ligation, or embolization.
Conflict of interest statement
The authors report no conflicts of interest. Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Funding
No financial support was received for this study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}