





Abstract
In skeletally immature people, chondroblastoma is an uncommon benign-appearing tumor that develops in the epiphysis of long bones. It is a kind of tumor that produces cartilage and makes up less than 1% of all bone cancers. Here, we report a case of a 23-year-old boy having chondroblastoma of the distal phalanx of the left great toe, which is an unusual site for the occurrence of chondroblastoma. Chondroblastoma is an exceptionally rare primary bone tumor that presents at the distal phalanx of the great toe.
Introduction
In skeletally immature people, chondroblastoma is an uncommon benign-appearing tumor that develops in the epiphysis of long bones. It is a tumor that produces cartilage and makes up less than 1% of all bone tumors [1]. In over half of the instances, it can continue into the metaphysis. Chondroblastoma often develops in the phalanx and is rare in the short bones of the hand and foot [2]. We describe a case of chondroblastoma in the left great toe’s distal phalanx, which was discovered via bone curettage and tumor removal.
Case presentation
A 23-year-old boy with swelling over his left great toe for 8 months came to the surgery outpatient department of a tertiary care hospital. The enlargement began slowly and has now grown to measure approximately 2.5 × 1.5 × 1.5 cm (Fig. 1).

Left great toe presentation with normal skin and nails surrounding the growth.
The skin and nails surrounding the growth are normal. It was linked to pressure-related discomfort. There was no history of trauma in the past. There was no fever or presence of any other comorbidity. A systematic assessment revealed no anomalies. Tests for renal function, plasma glucose, complete blood count, and other standard laboratory procedures were all within normal ranges. A radiographic examination reveals a coarse trabeculation and an osteolytic lesion in the great toe’s distal phalanx, which may indicate a benign bone malignancy (Fig. 2).

X-ray of the left foot.
Guided biopsy was taken and sent for histopathological examination but was inconclusive. A chondroblastoma diagnosis was taken into consideration as per radiological imaging, and the tumor was removed, and the great toe was disarticulated. The incision was marked and deepened in layers. Flaps were raised and friable, gritty, and decalcified bone was identified, and hence disarticulation of the left great toe was done (Fig. 3) and sent for histopathological examination. The postoperative course was uneventful. The patient was discharged on postoperative day (POD) 2 with sutures in situ. The patient came for follow-up after 10 days, and the suture line was found to be healthy with no active discharge or signs of inflammation and no restriction of movements. Sutures were removed on POD-10. Under a microscope, hematoxylin and eosin (low power mode) section shows immature chondrocytes (chondroblasts) round in shape with scanty cytoplasm, round nuclei with prominent nucleoli arranged into lobules separated by thin fibrous septae, and enclosed within a capsule suggestive of chondroblastoma (Fig. 4).
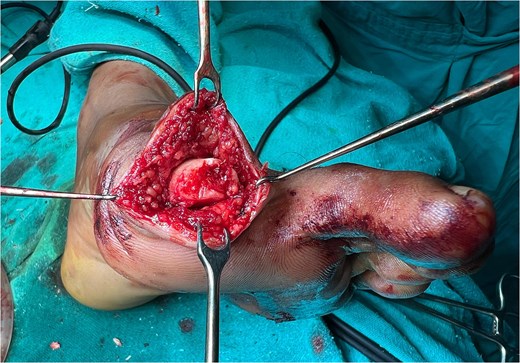
Intraoperative image.
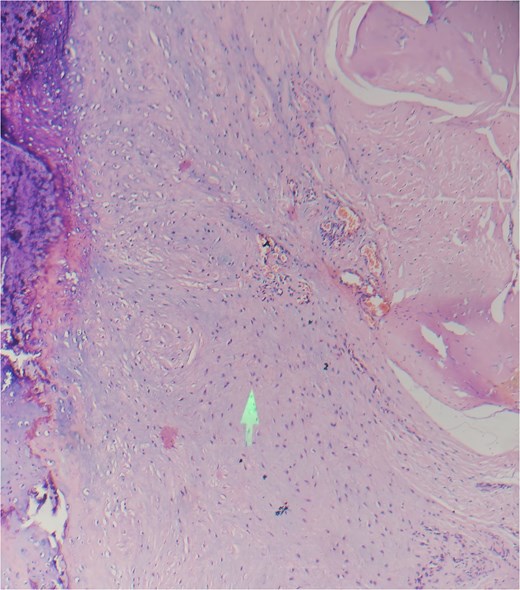
Hematoxylin and eosin (low power mode).
Discussion
Ewing originally described chondroblastoma as a calcifying giant cell tumor [3]. In young people, it typically manifests as a solitary, eccentric, round-to-oval lesion. It usually happens at the proximal humerus, distal femur, or proximal tibia [4]. Other unusual sites include flat bones such as the ribs, pelvis, vertebrae, scapula, and craniofacial bones [5]. Calcification has left the surface rough and chalky [6]. It was unusual for chondroblastoma to manifest on the great toe’s distal phalanx. Numerous investigations have determined that chondroblastoma originates from epiphyseal cartilage cells. Alternatively, as proposed by Brien et al., chondroid development in the adult population may be the result of multipotential mesenchymal cells found in tendon sheaths [7]. On a histological investigation, several mimics, such as giant cell tumors, chondromyxoid fibroma, aneurysmal bone cysts, and clear cell chondrosarcoma were distinguished [8, 9]. Although the histological signs of Chondroblastoma were classical in our case, a small number of patients also exhibit features such as cortical breach, soft tissue invasion, tumor necrosis, hemosiderin deposition, and secondary aneurysmal bone cyst formation [8, 10]. When a tumor’s excision is limited because of its location, the likelihood of the tumor returning is higher. The highest risk of tumor recurrence within 6 months to 8 years was found by Turcotte et al. in flat temporal bones. No evidence suggests that chondroblastoma resolves spontaneously; accordingly, surgical treatment is generally indicated.
Conclusion
Chondroblastoma is an uncommon primary bone tumor located in the long bones of young adults. Surgeons should take this tumor into consideration, although its presence at the distal phalanx of the great toe is extremely rare.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}