





Abstract
Hepatocellular carcinoma (HCC) is the second most common cause of cancer mortality worldwide. Liver resection is considered the pillar of curative treatment, although it is usually reserved for early-stage localized disease since the presence of metastases carries a poor prognosis. Despite advances in imaging, surgical techniques, and systemic therapy, the recurrence rate after oncologic resection remains high, even with localized disease. In the setting of extrahepatic HCC recurrence, there is no consensus regarding the best treatment strategy. Nevertheless, while the development of metastasis can be considered an expression of systemic disease, surgical resection may prolong survival. We report the case of a patient with a history of an oncologic hepatic resection for HCC, successfully treated with resection of an isolated peritoneal cavity metastasis. This case demonstrates that an aggressive approach involving the resection of extrahepatic HCC metastasis should be considered in select patients with the intention of achieving prolonged survival.
Introduction
Hepatocellular carcinoma (HCC) is one of the most common causes of cancer-related mortality worldwide [1–3] and has a poor long-term prognosis [3]. Liver resection is considered the gold standard treatment for eligible patients with localized disease, with a 5-year overall survival of 60%–80% [4]. Unfortunately, oncologic resection of HCC is still associated with a 5-year recurrence rate greater than 40% [3, 4]. Numerous authors have outlined that most recurrences appear quite early, generally between the two first years after initial treatment, and up to 90% of recurrent HCC cases are intrahepatic [3, 5, 6]. By contrast, isolated extrahepatic recurrence is relatively rare and is reported to be between 6% and 13% [1]. Late extrahepatic recurrence after initial treatment is even less frequent, with few published reports after 10 years [3, 5]. Extrahepatic metastatic recurrence is generally considered an incurable systemic disease, and the prognosis is poor due to limited effective treatments [7, 8]. Surgical resection in this setting remains controversial, given the lack of well-established guidelines. However, despite the published evidence of overall poor prognosis in this population, the literature does contain reports of surgery benefiting selected patients, resulting in prolonged survival [8–10].
We present the case of a patient with a history of HCC treated with an oncologic hepatic resection >10 years ago, presenting with a solitary extrahepatic abdominal metastasis successfully managed with surgical resection.
Case report
An 84-year-old female with an R0 oncologic hepatic resection for HCC 11 years ago presented with high alpha-fetoprotein (AFP) levels, followed by a computed tomography (CT) scan revealing a pelvic mass. After her index hepatic resection, she was managed with serial imaging and AFP tumor marker levels. The most recent AFP was elevated at 20.4 ng/ml, up from a previous value of 1.5 ng/ml one year earlier (normal range < 6.1 ng/ml). The CT demonstrated a 2.7 cm heterogeneous mass in the left lower quadrant, which was suspicious for a neoplasm. (Figs 1 and 2) The patient denied having abdominal symptoms, and the mass was not palpable during the physical exam.
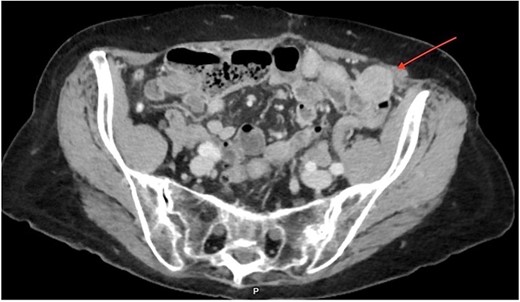
CT imaging of the pelvis (axial section) displaying a rounded 2.7 × 2.7 cm heterogeneous mass localized in the left anterior pelvic cavity, near the colon wall, without peripheral enhancement.

CT imaging of the pelvis (sagittal section) displaying the left localization of the 2.7 × 2.7 cm heterogeneous pelvic mass.
Image-guided needle biopsy of the pelvic mass was attempted; however, at the time of the procedure, the mass mobility made it impossible. Due to suspicion of potential involvement of the colonic wall, a colonoscopy was performed, which was unremarkable. A positron emission tomography scan confirmed the CT findings, exhibiting a rounded mesenteric nodule in the left quadrant measuring 2.6 cm, with elevated Fludeoxyglucose F18 (FDG) tracer uptake (Fig. 3).
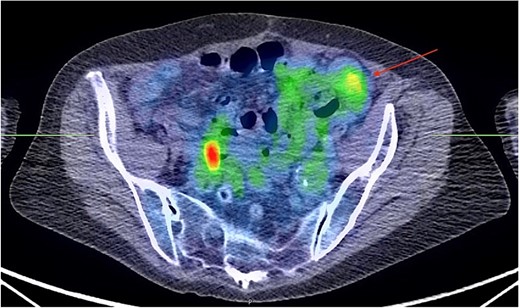
PET scan showing a rounded nodule within the anterior mesentery in the left pelvis measuring 2.6 × 2.6 cm in size. It has a moderate tracer uptake with peak SUV of 3.6. (arrow). No other mesenteric nodules are identified. The image visualized on the right pelvis was considered a normal physiologic uptake within the bowel.
Given the concern for HCC extrahepatic metastasis, and since there was no evidence of other organ involvement, surgical resection was planned. Initially, a diagnostic laparoscopy was performed to evaluate for any evidence of occult metastatic disease elsewhere in the peritoneal cavity. This was followed by a laparoscopic resection of the intraabdominal mass, identified as a round, well-circumscribed lesion in the left lower quadrant. An en-bloc resection was completed with a gross margin of at least one centimeter. The specimen was removed in a bag to minimize the risk of seeding the abdominal wall. Pathologic analysis demonstrated a well-differentiated 3.0 cm HCC with lymphovascular invasion, consistent with metastatic disease. The patient’s postoperative course was uncomplicated. At a 2-year follow-up, the patient remains without imaging or biochemical evidence of disease.
Discussion
HCC is a malignant neoplastic disease often portending a poor long-term prognosis at the time of diagnosis [3]. It accounts for 80% of all forms of liver cancer cases [1], with a reported 5-year recurrence rate that exceeds 40% [3, 4]. HCC is commonly spread by hematogenous or lymphatic pathways and, locally, by direct invasion of adjacent structures and organs. Among the recurrences, intrahepatic relapse accounts for 66%–90% of the cases. Extrahepatic recurrence is less common, representing 6%–13% of recurrences [8, 11–13]. The lung is the most common metastatic site [14], followed by the peritoneum, bones, and adrenal glands [5]. Several factors have been associated with an increased likelihood of developing extrahepatic metastasis. Ochiai et al. [12] analysed patients who developed extrahepatic recurrence after R0 HCC resection and compared them to those who remained disease-free for at least 5 years. They found that extrahepatic metastasis were significantly associated with age (57.2 ± 11.6) and hepatic involvement of primary tumor beyond one subsegment, among others. Natsuizaka et al. [15] reported that NM+ and advanced intrahepatic tumor stages were observed more frequently at the diagnosis of HCC in these patients. Our patient was over 60 years old; the tumor involved segments 5 and 6 and was classified as T4.
Extrahepatic metastasis carries a worse prognosis compared with those with isolated local disease, with a 12-month survival rate between 21% and 25% [7]. Conversely, intrahepatic metastatic lesions have a reported 5-year overall survival rate of 60%–80% [4]. Most recurrences develop early, within the first two years after initial treatment [5, 6]. Late recurrence is comparatively rare, with only a few existing case reports. Wong et al. [3] and Kim et al. [5] reported extrahepatic recurrence of HCC after 12 and 28 years, respectively. Our case report shows recurrence after 11 years. While liver resection is considered the mainstream curative treatment for eligible patients with intrahepatic HCC recurrence [4], the best treatment option for extrahepatic metastasis remains controversial, and it is often considered a terminal-stage disease [8]. However, more aggressive surgical treatment has been employed in certain scenarios to prolong survival [7]. Several studies have demonstrated that surgical resection (SR) of extrahepatic metastasis may benefit selected patients with HCC [8, 14]. Chan et al. [8] retrospectively reviewed the medical records of 140 patients with extrahepatic metastasis of HCC and evaluated the outcomes of those who had undergone SR. The survival rates of these patients were significantly improved compared with those who did not have SR, with one and 3-year survival rates of 24% and 7%, respectively, while the non-surgical group survival rates were 8% and 0%, respectively. Other authors [12] have also shown that resection of the recurrent tumor was the only independent favorable factor associated with survival in patients with extrahepatic recurrence.
While the optimal management strategy for extrahepatic metastasis of HCC remains under investigation, emerging evidence suggests that surgical resection could offer a survival advantage for a select group of patients. Analysing patient characteristics may allow the identification of this population, which could lead to establishing specific criteria that could elevate surgical resection as a preferred treatment modality for extrahepatic metastasis of HCC.
Conflict of interest statement
None declared
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.

{kind=link}
{kind=link}
{kind=link}