





Abstract
Left-sided gallbladder (LSG), also known as sinistroposition, is a rare congenital anatomical variation in which the gallbladder is located to the left of the round ligament (ligamentum teres). This anomaly is usually asymptomatic and frequently detected incidentally during surgery, but it may pose significant technical challenges and increase the risk of intraoperative bile duct injury. We report a rare case of a 58-year-old male with symptomatic cholelithiasis in whom a LSG was unexpectedly identified during elective laparoscopic cholecystectomy. The operative strategy was modified by trocar repositioning to achieve adequate exposure and safe dissection. The procedure was completed successfully without intraoperative or postoperative complications. This case highlights the importance of intraoperative vigilance and flexible surgical strategies when encountering unexpected hepatobiliary anatomical variations.
Introduction
Left-sided gallbladder (LSG), also known as sinistroposition, is a rare congenital anatomical variation characterized by displacement of the gallbladder to the left of the round ligament without situs inversus [1, 2]. The reported incidence ranges from 0.04% to 0.7%, and most cases are discovered incidentally during hepatobiliary surgery performed for unrelated biliary pathology [3, 4]. Although usually asymptomatic, LSG is frequently associated with biliary and vascular variations that may increase the risk of bile duct injury during laparoscopic cholecystectomy [5].
Previous studies have shown that LSG is often accompanied by abnormal cystic duct insertion and portal venous variations, which may obscure the critical view of safety and complicate surgical dissection [6, 7]. Because preoperative diagnosis remains challenging and LSG is commonly not detected on routine ultrasonography, intraoperative recognition and appropriate modification of surgical strategy are crucial for preventing iatrogenic bile duct injury [6, 7].
Herein, we report a rare case of LSG unexpectedly encountered during elective laparoscopic cholecystectomy for symptomatic cholelithiasis. We describe the intraoperative findings, technical modifications and postoperative outcomes, and review the relevant literature to highlight practical considerations for the safe management of this uncommon anatomical variation.
Case presentation
A 58-year-old male presented with dull, intermittent right upper quadrant and epigastric pain, occasionally related to fatty meals. He reported similar episodes in the past that had been diagnosed as gastritis and managed conservatively. During the current admission to the hospital, his symptoms recurred. Physical examination revealed mild epigastric tenderness without peritoneal signs. Laboratory investigations, including liver function tests, were within normal limits. Abdominal ultrasonography revealed gallstones without signs of acute cholecystitis, and the common bile duct was of normal diameter; the gallbladder was reported in a normal position, with no specific evaluation for ectopic location (Fig. 1). Therefore, elective laparoscopic cholecystectomy was indicated.
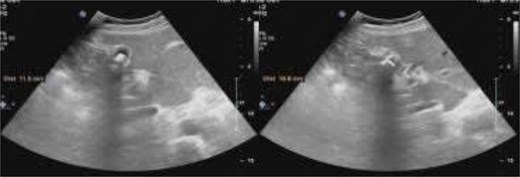
Preoperative ultrasonography demonstrated gallstones, with a normal-caliber common bile duct; the gallbladder was reported in a normal position and ectopic location was not specifically assessed.
The procedure was initiated using our routine three-port technique, including a 10-mm umbilical camera port, a 10-mm epigastric working port, and a 5-mm right subcostal port. Upon laparoscopic exploration, the gallbladder was unexpectedly identified to the left of the round ligament (Figs 2 and 3a). To facilitate adequate exposure and safe dissection, the epigastric trocar was repositioned to the left side (Fig. 3b). The gallbladder was mildly inflamed and adherent to the omentum. After repositioning of the epigastric trocar, meticulous dissection was performed and the Critical View of Safety was fully achieved before clipping and division of the cystic duct and artery. No bailout strategy such as fundus-first dissection or subtotal cholecystectomy was considered necessary, and intraoperative cholangiography was not required because the biliary anatomy was clearly identified. The operative time was 70 minutes, and the procedure was completed without intraoperative complications. The postoperative course was uneventful and the patient was discharged on postoperative day two. He returned to work on postoperative day five.
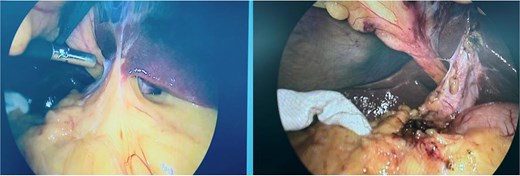
The greater omentum adherent to the inflamed gallbladder, shown before and after adhesiolysis.
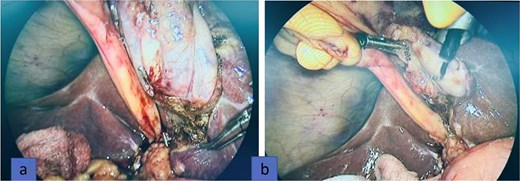
Intraoperatively, the gallbladder was found entirely to the left of the round ligament without situs inversus (a). The epigastric trocar was repositioned to the left of the falciform ligament to improve exposure and facilitate dissection (b).
Discussion
LSG, or sinistroposition, is a rare congenital anatomical variation in which the gallbladder is located to the left of the round ligament in the absence of situs inversus [1]. Because patients usually present with symptoms indistinguishable from conventional gallstone disease, LSG is most often diagnosed incidentally during laparoscopic cholecystectomy [8]. Routine ultrasonography is primarily useful for detecting gallstones and frequently fails to identify abnormal gallbladder positioning, resulting in limited preoperative recognition of this anomaly [8].
Embryologically, LSG is thought to arise from abnormal migration of the gallbladder primordium or altered hepatic rotation during development, leading to atypical biliary and vascular anatomy [6]. Several studies have demonstrated that LSG is commonly associated with abnormal cystic duct insertion and variations of the portal venous and hepatic arterial systems, which may significantly increase the risk of bile duct injury during laparoscopic cholecystectomy [6, 9].
From a surgical perspective, distorted anatomical landmarks and a short cystic duct and artery frequently make dissection technically demanding in patients with LSG [7, 10, 11]. Modification of trocar placement, particularly repositioning of the epigastric port to the left side, has been consistently recommended to improve exposure and facilitate safe dissection [8, 10]. Strict adherence to the Critical View of Safety remains the cornerstone of preventing bile duct injury in these patients [11]. In cases with unclear biliary anatomy, selective use of intraoperative cholangiography may further enhance operative safety [12].
In the present case, the gallbladder was located entirely to the left of the falciform ligament, and the cystic duct and artery were short but clearly visualized. Repositioning of the epigastric trocar allowed for adequate exposure and safe dissection, enabling completion of the procedure without complications. These findings are consistent with previously reported case series and reviews emphasizing that individualized port placement, meticulous dissection, and strict implementation of the Critical View of Safety are key determinants of successful laparoscopic management of LSG [8, 10].
Overall, awareness of LSG and careful intraoperative adaptation are essential for preventing iatrogenic bile duct injury and ensuring optimal surgical outcomes, even during routine elective laparoscopic cholecystectomy.
Conclusion
LSG is a rare but clinically important anatomical variation that may significantly increase the risk of bile duct injury during laparoscopic cholecystectomy. Because preoperative diagnosis remains challenging, surgeons should maintain a high index of suspicion when encountering unexpected biliary anatomy. Strict adherence to the Critical View of Safety, individualized trocar placement and flexible intraoperative adaptation are essential to ensure safe dissection and optimal surgical outcomes.
Author contributions
All authors contributed to the study conception and design. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Conflicts of interest
The authors declare no conflicts of interest.
Funding
No funds, grants, or other support were received during the preparation of this manuscript.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.

{kind=link}
{kind=link}
{kind=link}