





Abstract
Calcified amorphous tumors are extremely rare benign cardiac lesions that can emerge in any chamber, and have many clinical obscurities. We herein report a case of a mid-aged previously healthy male with a complaint of recurrent chest pain. Echocardiogram revealed the presence of right atrial mass that was confirmed by transesophageal echocardiography. The patient underwent total resection of the mass with attached atrial wall. Pathological studies confirmed the diagnosis of calcified amorphous tumor. Five-year follow-up was uneventful with total symptomatic relief. In conclusion, we recommend considering the diagnosis of calcified amorphous tumors in any patient with intracardiac mass.
INTRODUCTION
Calcified amorphous tumors of the heart (CATs) are rare cardiac masses that develop in any cardiac chamber [1]. CATs account for 2.48% of all primary cardiac tumors [2]. The clinical presentation varies greatly, and is attributed mainly to embolization or obstruction depending on the size and the location [3]. Although the pathogenesis is not fully understood, all lesions have similar microscopic appearance of nodular deposits of calcium within a background of eosinophilic, amorphous and fibrinous material [1]. CATs are associated with valvular heart diseases, coronary artery disease and end-stage renal disease [3]. The detection of these tumors is often incidental, and complete surgical excision is the preferred management; however, recurrence remains possible following surgical excision [3, 4]. Since the full etiology is obscure, emerging cases of calcified amorphous tumors should be further studied to fully understand the clinical characteristics of the disease. We, herein, present a case of a CAT in the right atrium in a 37-year-old man presented with recurrent chest pain.
CASE PRESENTATION
A 37-year-old Caucasian male presented with a complaint of non-exertional left-sided parasternal chest pain recurring over the past 4 months. The pain lasts for 10–15 min and is accompanied by nausea and diaphoresis. The patient also reported episodes of presyncope lasting for 3–15 min, and one episode of sudden severe dyspnea with mild hemoptysis. Past medical and family history is unremarkable. He does not take any regular medication. Vital signs and physical cardiovascular examination were normal.
Resting and pain-related electrocardiogram, chest X-ray, pulmonary function tests, carotid ultrasound examination and full laboratory workup were normal. Brain computerized tomography was normal.
Transthoracic echocardiography demonstrated an irregular right atrial mass attached to the atrial wall with wide base near the atrial connection with the inferior vena cava (IVC) causing partial IVC dilation without significant flow obstruction. In addition, there was a mild tricuspid regurgitation and systolic pulmonary pressure measured 47mmhg (Fig. 1a).
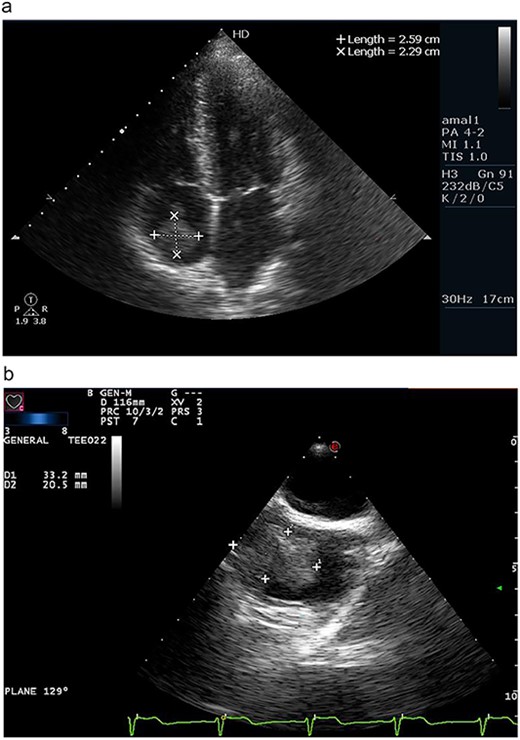
(a) Apical four chamber view on transthoracic echocardiography revealing a right atrial mass measuring 2.59 × 2.29 cm. (b) Transesophageal echocardiography confirming the presence of wide-based, irregular and lobulated right atrial mass measuring 3.32 × 2.05 cm.
On transesophageal echocardiography, the mass appeared lobulated, attached to the right atrial wall and containing multiple foci of calcifications (Fig. 1b).
Multi-slice computerized tomography with contrast injection of the neck, chest, abdomen and pelvis was normal, except for the presence of a filling defect inside the right atrium at the connection site of the IVC, which was consistent with the findings of echocardiography. Coronary angiography was normal.
The patient underwent sternotomy, femoral vein was isolated and cannulated, the aorta and superior vena cava were cannulated; the pericardium was incised, and the patient was connected to the cardiopulmonary bypass machine. The right atrium was incised longitudinally, and the mass was totally resected along with the attached wall and adjacent part of the IVC; then atria was closed on two layers with the use of pericardial graft to prevent IVC entrance stenosis. Temporary pacemaker was placed. The pacemaker was removed safely and the patient was discharged on day 4 in a good status.
On gross examination, the resected mass appeared irregular in shape, white-gray in colour and measured 33.2 × 20.5 cm in size. Microscopic studies demonstrated a wide eosinophilic degenerated fibrin background, with many irregular and nodular calcified deposits. Additionally, small foci of myxoid mixture associated with bland spindle cells and scattered collections of foamy histocytes were observed, confirming the diagnosis of calcified amorphous tumor (Fig. 2).
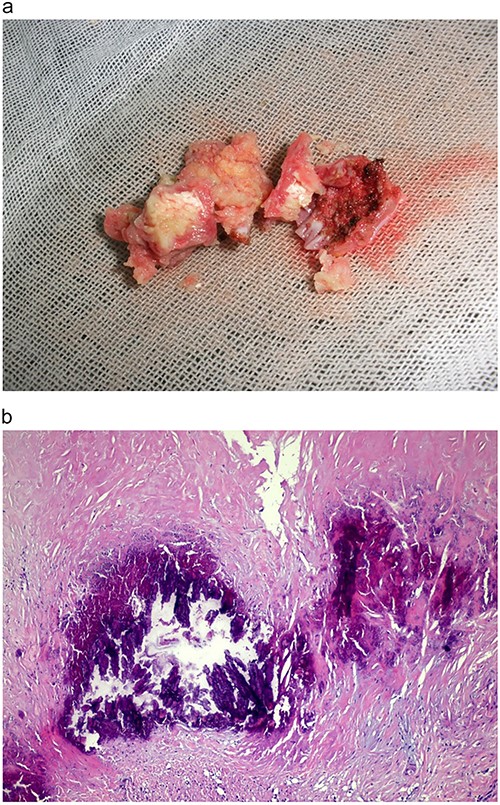
(a) Gross view of the resected tumor appearing irregular, soft and measuring 3 × 2.5 × 2 cm. (b). Microscopic image of the tumor specimen demonstrating wide eosinophilic degenerated fibrin background, with many irregular and nodular calcified deposits; small foci of myxoid mixture associated with bland spindle cells and scattered collections of foamy histocytes.
Postoperative follow-up based on detailed clinical examination and transthoracic echocardiography (after 1 month, 6 months, 1 year and 5 years) was uneventful. Postoperative transthoracic echocardiography demonstrated normal-sized right chambers, mild to moderate tricuspid regurgitation, IVC dilation and systolic pulmonary pressure of 37 mmhg.
DISCUSSION
Primary cardiac tumors have an extremely low incidence rate of 0.0017–0.02% of all cardiac tumors. Ninety percent of cardiac tumors are benign, with myxomas being the most common type accounting for 50% of cases [2]. Cardiac CATs are an extremely rare type of non-neoplastic primary cardiac tumors accounting for 2.48% of all primary cardiac tumors [5]. It was reported for the first time in 1997 by Reynolds et al. [1], and only a handful of cases have been reported ever since.
CATs present as a hypodensive mass within an amorphous degenerating fibrinous background. They can emerge in any part of the four chambers of the heart. The most common locations are the mitral valve or annulus followed by the right atrium, with only 20 reported cases in the literature (including ours) [3, 6].
Signs and symptoms vary depending on the size, location, rate of growth and associated comorbidities of the tumor, ranging from shortness of breath to pulmonary embolism, cerebrovascular accidents and heart failure [3].
According to the age of presentation, multiple symptoms should be considered under diagnosis. Dyspnea and syncope were among the most common symptoms reported in adults, in addition to embolization or obstruction-related symptoms, whereas in this case, the presentation was recurrent chest pain, which is an extremely rare and has only been reported in a couple of cases described as funny sensation in the chest [3]. Symptoms mimicking angina can hinder the early diagnosis of CATs. Neonates can present with tachypnea, cyanotic attacks and heart murmurs [7, 8].
CATs are most commonly associated with valvular diseases with a prevalence of (31%), followed by end-stage renal disease (21%), diabetes (14%) and coronary artery disease (12%), respectively [3].
Although CATs are often asymptomatic and discovered by routine check-up, surgical resection remains the ultimate diagnostic and therapeutic procedure, as CAT might lead to detrimental consequences attributed to obstruction or embolization, and postoperative recurrence is highly unlikely and have only been reported with incomplete excision [4].
Surgical intervention is usually curative and there is no special approach required; however, in the case of underlying valvular disease or enlarged obstructive tumor, valve replacement is recommended. In our case, the size of the tumor is consistent with the reported average size of CATs (29 × 17 mm3), and was completely resected along with the attached atrial wall and the adjacent part of the IVC to fix its dilation.
The prognosis is generally good following complete resection of the mass, and follow-up imaging is recommended [3].
To conclude, we recommend considering the diagnosis of calcified amorphous tumors in any patient with intracardiac mass.
ACKNOWLEDGEMENTS
We would like to thank Dr A. Salah Koja and Dr Vairy Rezkallah for their support during this work.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
There are no funding or financial support offered or used for this work.

{kind=link}
{kind=link}