





Abstract
Among intraabdominal lymphangiomas, colonic lymphangiomas are rare. These cystic tumors are generally asymptomatic and incidentally found but may present with bleeding or obstructive symptoms. Intussusception by such tumors is scarcely reported, with only nine previously reported cases listed in Pubmed. We report a case of a 41-year-old female Asian patient who presented with acute abdomen and was diagnosed with colonic intussusception caused by lymphangioma. She received emergent right hemicolectomy, recovered well without complications, and was discharged on the 5th postoperative day.
Introduction
Lymphangiomas are benign cystic neoplasms of lymph vessels, commonly occurring in the head and neck or axilla of pediatric patients. These tumors are mostly congenital but may arise spontaneously during adolescence or adulthood. Lesions of various locations have been reported, and in the abdominal cavity, cases of lymphangiomas originating from the pancreas, spleen, mesentery, ovaries, and retroperitoneum have been mentioned in previous literature.
Colonic lymphangiomas are rare and are commonly found as submucosal tumors incidentally found upon imaging. Symptoms may arise due to cyst rupture, bleeding, and rarely, obstruction. A few cases of intussusception with colonic lymphangiomas as the leading point have been reported, with all cases having undergone surgical resection.
Here we present a case of a 41-year-old Korean female patient who underwent laparoscopic right hemicolectomy for colonic intussusception caused by a cystic tumor, pathologically confirmed as a lymphangioma.
Case report
A 41-year-old female with no previous medical conditions or operation history was referred to the emergency department with diffuse lower abdominal pain which began 3 days prior. The patient also suffered severe watery diarrhea for which she visited a local hospital and took a computed tomography (CT) scan. Imaging showed a cystic mass as a leading point of a right sided colonic intussusception, and she was referred to our department for surgery.
Initial vitals were normotensive and stable, without fever. Physical examination indicated mild lower abdomen tenderness, but the abdomen was rather soft and not distended or tympanic. Laboratory tests were all within normal limits except for the white blood cell differential count, showing an elevated segmented neutrophil ratio of 89.4%. Formal CT readings highlighted a 6.2 cm sized septated cystic tumor of the right colon as the leading point of the colonic intussusception (Fig. 1). Radiologists suggested a differential diagnosis of duplication cyst, mucocele, endometriosis, lymphangioma, or myxoma.

Initial CT scan of the colo-colic intussusception and the septated cystic tumor.
Based on these findings, an emergent laparoscopic exploration and right hemicolectomy was performed. Complete mesocolic excision was done as we could not rule-out the possibility of malignancy such as malignant mucinous neoplasm around cecum and appendix. Five ports (one 12 mm camera port, one 5 mm working port, and three 3 mm working ports) were used, and upon exploration, the cystic lesion appeared as a blueish gray, round lesion causing intussusception (Fig. 2). Specimen extraction and extracorporeal side to side ileocolic anastomosis was done by extension of the umbilical camera port into a mini laparotomy of ~4 cm. Drains were not inserted, and the skin was closed with intradermal vicryl sutures then glued with skin bond. A large 7 × 5 cm2 sized submucosal cyst could be seen in the specimen (Fig. 3).
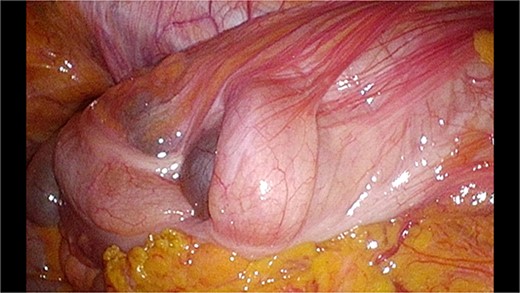
Laparoscopic view of the colo-colic intussusception.
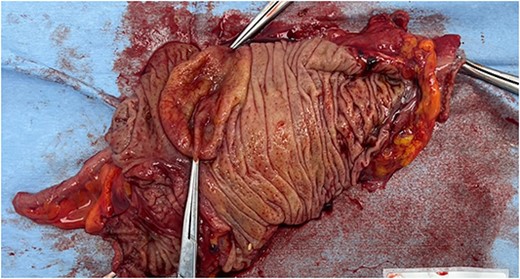
The cystic tumor on the fresh specimen.
Postoperatively, the patient experienced no complications and was discharged on postoperative Day 5. She was followed up to our outpatient clinic 2 weeks later, without any problems.
Pathologic review showed multiple cysts in the right colon wall submucosa, lined by a single layer of bland, flat cells, and devoid of red blood cells in the lumen. For definitive diagnosis, additional immunohistochemistry stains were done. Results showed positive CD31 and D2-40 expression in the thin endothelial cells lining the cyst, suggesting a tumor of lymphatic origin. Thus, we concluded that the lesion was a cystic lymphangioma.
Discussion
Colorectal lymphangiomas often presents as a submucosal tumor covered in normal mucosa. Macroscopically these lesions have a yellow or grayish yellow–pink color with multiple cysts containing watery fluid content. They may be classified as one of the following: simple (capillary), cavernous, or cystic lymphangiomas with the cystic type being the most common. The precise pathophysiology is yet to be described and proved, but Matsuda et al. [1] suggested that excessive proliferation of endothelium in the wall of lymphatic vessels may be caused by inflammation, traumatic stimulus, or radiation in a Japanese review of 279 cases.
The vast majority of colorectal lymphangiomas have been reported in eastern countries, with 85% percent of cases having been reported from Japan until 2007. This disease has a slight male predominance, with a 1.4–1.6 times higher prevalence in males compared to females. Symptoms, when present, are often vague and non-specific. Abdominal pain, hematochezia, or obstructive symptoms may arise depending on the size and location of the lesion [2]. In some cases, other complications such as anemia, infection, protein losing enteropathy, [3] and intussusception have been reported.
Initial presentation requires differential diagnosis with other cystic tumors such as mucoceles, intestinal duplication cysts, and rarely cystic degeneration of solid tumors such as adenocarcinoma or gastrointestinal stromal tumors [4]. In this case, the initial radiologic report also suggested an appendix mucocele or ileal duplication cyst as the leading point of the intussusception. Appendiceal or cecal intussusception with the appendix as a leading point is surprisingly more frequently seen than one might expect, as pointed out by Chaar et al. [5] in their review of literature in 2009. They counted 191 cases of intussusception reported in PubMed. Endometriosis, appendiceal mucoceles, and simple appendicitis were the three most frequent causes in adults. Going into the operating room, we also considered appendix mucocele to be the most likely cause.
There are only nine previously reported cases of intussusception caused by colorectal lymphangiomas in current literature searched on PubMed, from 1975 to 2019 [6–14], listed with details in Table 1. Two early reports (1975, 1988) were not reviewable. Of the other seven cases, four patients were female and three were male. Mean age was 33.3, with the youngest patient being 16 years old and the oldest 45 years old. Only one patient had a history of operation for uterine myoma, and the rest were healthy and had no medical conditions. Symptoms included abdominal pain, bowel habit change, hematochezia, and vomiting. Two cases involved the descending colon, and the rest were located in the right colon, more specifically the ileocecum. Three had right hemicolectomy, two had ileocecectomy, one had anterior resection, and one had segmental resection. Apart from the anterior resection, all other surgeries were done by laparotomy.
Previously reported nine cases of colonic intussusception caused by lymphangioma.
| Reference | Year | Age/Sex | Race | History | Symptom | Initial mode of diagnosis | Area | Size (cm) | Operation |
|---|---|---|---|---|---|---|---|---|---|
| [12] | 1975 | Unspecified | |||||||
| [14] | 1988 | Unspecified | |||||||
| [11] | 1998 | 28/F | Asian | None | Acute abdominal pain, vomiting | CT, US | Cecum | 7 | Emergent right hemicolectomy |
| [6] | 2003 | 39/F | Asian | Myomectomy | Acute abdominal pain | US, CT | Ileocecal | 9×6 | Emergent ileocecectomy |
| [13] | 2005 | 16/M | Asian | None | Acute abdominal pain, hematochezia | CT, US | Ileocecal | 6×3 | Emergent right hemicolectomy |
| [3] | 2006 | 32/F | Asian | None | Hematochezia | CT, colonoscopy | Descending colon | 5×3 | Emergent segmental resection |
| [9] | 2009 | 45/M | Asian | None | Chronic abdominal pain, diarrhea | Colonoscopy | Ileocecal | 3×3 | Emergent right hemicolectomy |
| [10] | 2011 | 30/F | Asian | None | Acute abdominal pain | US, CT | Cecum | 9 | Emergent ileocecectomy |
| [7] | 2019 | 43/M | Caucasian | None | Chronic abdominal pain, bowel habit change | CT, colonoscopy | Descending colon | 1.3×1 | Elective laparoscopic anterior resection |
| Present | 2023 | 41/F | Asian | None | Acute abdominal pain | CT | Ileocecal | 7×5 | Emergent laparoscopic right hemicolectomy |
CT: computed tomography; US: ultrasonography
Our patient was a healthy female in her 40s, with no history of abdominal trauma or inflammatory disease. Interestingly, she was taking routine screening examinations annually at an advanced screening center, including annual abdominal sonography and colonoscopy. The last of these screening sessions was only 4 months before the onset of intussusception, and no abnormality was detected. It is important to note that the lesion was not detected upon screening colonoscopy. This might have been caused by mucosal stretching due to gas inflation, hiding the lesion.
Small uncomplicated, pedunculated lesions may be resected endoscopically with snare electrocautery or ligation loops. One case reported ligation of a lesion as large as 5 cm, but this was likely possible due to the pedunculated nature of the tumor [15]. More than size, the shape of the mass is likely to influence resectability under endoscopy and an attempt to endoscopically resect a smooth sessile subepithelial tumor is not encouraged as risk of perforation is too high. Simple unroofing of the tumor has been reported, but hypothetically this may cause continuous lymphatic leakage into the intestinal lumen which may result in protein losing enteropathy.
To date there are no reports of colorectal lymphangiomas transforming into malignant lesions. There is, however, a case that reported a right inguinal lymphangioma recurring multiple times with the endothelial cells developing atypia, suggesting transformation into a lymphangiosarcoma [16]. Additionally, there have been two reports of recurred intraabdominal lymphangiomas >10 years after the first surgery without any pathologic evidence of malignant features [17, 18]. Whether these were the result of incomplete resection, which is known to be a risk factor for lymphangioma recur, is not described. With such little evidence of malignant transformation or recur after complete resection, lymphangiomas are considered to be benign lesions.
Whether oncological surgery such as the right hemicolectomy with complete mesocolic excision done in this patient is necessary in this setting is debatable. Marinis et al. [19] reported that up to 30% of adult small bowel intussusceptions, and 66% of adult colonic intussusceptions were caused by malignancy. Considering this if the preoperative diagnosis is not solid complete oncological resection seems logical. With the growing evidence of safe laparoscopic surgery for colorectal cancer [20], we encourage that laparoscopic resection to be considered first if not contraindicated (for reasons such as severe bowel dilatation or panperitonitis due to perforation).
For the final diagnosis of a cystic lymphangioma, subepithelial lesions with a flat and thin single layered endothelial lining are typical findings. Immunohistochemical staining with monoclonal antibodies CD31 and D2–40 are consistently positive and more than half show positive results with CD34 staining.
To conclude, we presented a case of a 41-year-old female patient that acutely presented with right colon intussusception caused by colonic lymphangioma that was not detected despite extensive screening. Laparoscopic right hemicolectomy was done without any complications, and pathology confirmed cystic lymphangioma. Having reviewed the current literature, cystic lymphangiomas causing intussusception mainly occurred in the Asian population, with large (>3 cm) tumors of the right colon requiring emergent ileocecectomy or right hemicolectomy. Small pedunculated lesions without complications may be selected for endoscopic removal, but larger or smooth sessile tumors should be surgically resected. Given the differential diagnosis in an acute emergent setting of intussusception, oncologic surgical resection is logical, and pathology must be confirmed.
Conflict of interest statement
None declared.
Funding
None declared.
References
Yu H, Mao Q, Zhou L, Li J, Xu X.

{kind=link}
{kind=link}
{kind=link}