





Abstract
The coexistence of ectopic kidney with locally advanced rectal cancer is rare. It poses a surgical and oncological challenge for the treating team. Careful preoperative surgical planning and decision about the neoadjuvant treatment are paramount.We report a 40-year-old male newly diagnosed with rectal adenocarcinoma with ectopic kidney. His preoperative staging was T3N2M0 with ectopic malrotated left kidney. After discussion in the multi-disciplinary team meeting, decision was to omit the neoadjuvant treatment and to go for low anterior resection. The procedure started open, and the findings showed the kidney lying in retroperitoneum around 3 cm above the peritoneal reflection and was separable from the tumor. Oncological resection of the rectosigmoid colon by lateral to medial approach with separation and preservation of the kidney, an end-to-end stapler anastomosis followed with a protective loop ileostomy. The patient had a smooth postoperative course, and the final pathology was T3N1Mx. He received eight cycles of adjuvant XELOX and was free of diseases on 1 year follow-up. There is no optimal option in managing this scenario due to a highly variable blood supply of the ectopic kidney and rarity of this condition. Multi-disciplinary team meeting with preoperative radiological mapping and patient counseling is crucial in making the best decision.
INTRODUCTION
An ectopic kidney is a failure of migration of the kidney to it is normal position during the fetal development; instead, it remains in the pelvis. The incidence of this condition is reported to be one in 2100–3000 cases making it a rare condition [1, 2]. It is estimated that the incidence of rectal cancer is 44 180 in the United States on 2019 [3]. The coexistence of ectopic kidney with rectal cancer makes the condition more complex in surgical planning and the need for radiotherapy in locally advanced disease. Here in this case report, we present a case of an ectopic kidney with a locally advanced rectal cancer (T3N1M0) along with discussing the importance of perioperative management and surgical planning.
CASE REPORT
A 40-year-old male, deaf and mute presented with 4 months history of bleeding per rectum associated with a change in bowel motion, and there was no abdominal pain, no history of weight loss and no family history of colorectal cancer, nor history of tobacco use. On clinical assessment, he looked pale with normal vital signs and his examination showed soft abdomen, no tenderness or palpable masses with per rectal exam revealed blood but no palpable tumor.
The basic lab Investigation showed Hgb level of 8.6 g/dL and CEA level of 4.8 ng/ml. On further investigation, colonoscopy revealed a large friable fungating circumferential rectal mass at 9 cm from anal verge extending to the distal sigmoid colon, it was nonobstructing with a length of 8 cm and the rest of the colon was normal. A biopsy from the mass was taken and showed invasive moderately differentiated adenocarcinoma. On further routine of radiological staging, CT of the chest, abdomen and pelvis confirmed the upper rectal mass with ectopic malrotated left kidney located in the lower abdomen and upper pelvis, opposite to L5-S1 vertebral bodies (Figs 1 and 2). There was no peritoneal disease or distant metastasis. Moreover, MRI pelvis showed again an upper rectal mass with mesorectal fat invasion and multiple lymph nodes (T3N2) and confirmed an ectopic left kidney (Figs 3 and 4).
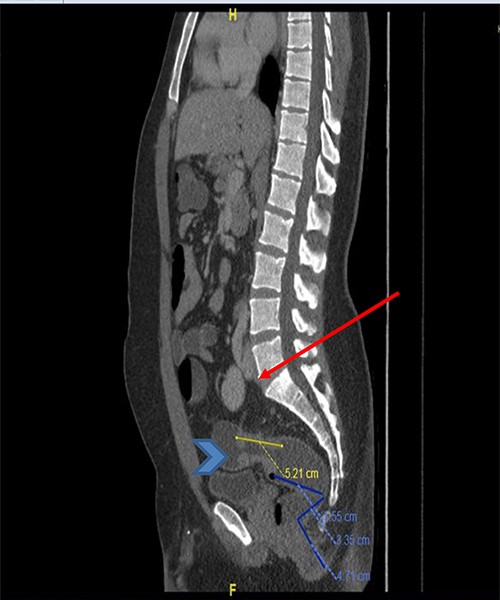
CT scan of the abdomen and pelvis (sagittal view) showing the upper rectal mass (arrowhead) with ectopic kidney (arrow).
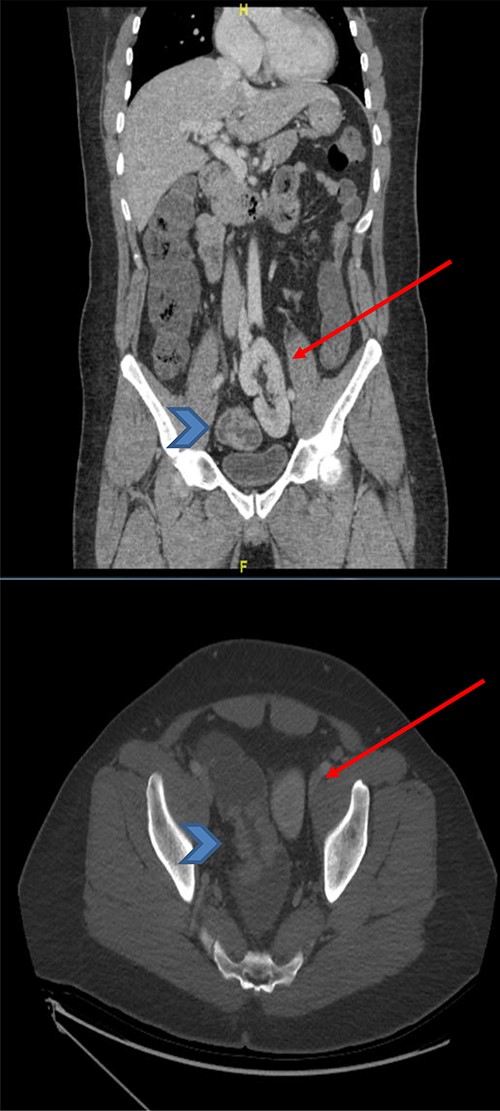
CT scan of the abdomen and pelvis (coronal and axial view) showing the upper rectal mass (arrowhead) with ectopic kidney (arrow), clear plane noted in-between without tumor invasion.
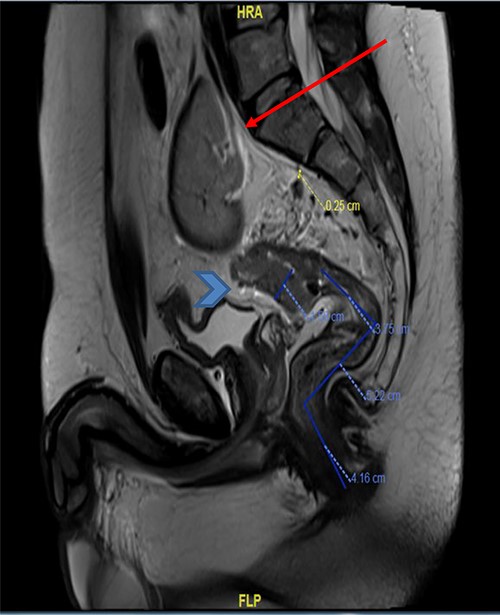
MRI pelvis (sagittal view) showed upper rectal mass with mesorectal fat involvement (arrowhead) and ectopic pelvic kidney (arrow).
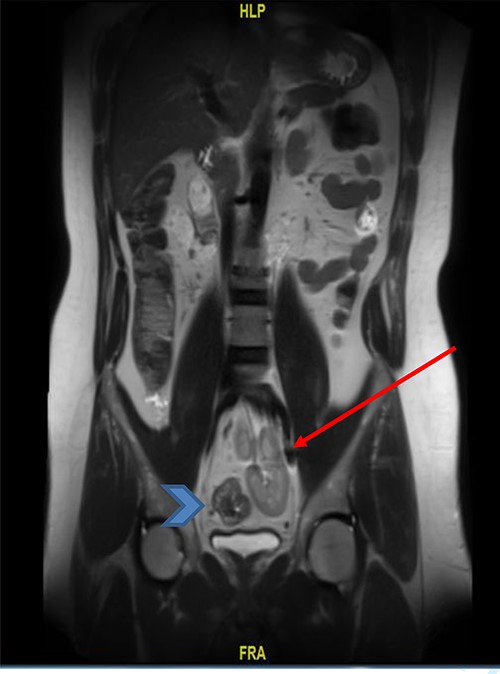
MRI pelvis (coronal view) showed upper rectal mass with mesorectal fat involvement (arrowhead) and ectopic pelvic kidney (arrow).
The case was discussed in a multi-disciplinary meeting and the decision was to omit the neoadjuvant radiotherapy due to the location of the kidney and to go for upfront surgery then adjuvant chemotherapy. An open low anterior resection was carried on from the beginning and intraoperative findings showed the left ectopic kidney lying around 3 cm above the peritoneal reflection in the retroperitoneal space and it was separated from the tumor. The procedure continued with lateral to medial mobilization of the colon, separating the kidney from tumor, followed by oncological resection of the rectosigmoid with ligation of the inferior mesenteric artery and veins. The bowel continuity restored with stapler end-to-end anastomosis and a protective loop ileostomy was created by the end of the procedure. The patient had a smooth postoperative course and was discharge from the hospital on Day 5 post-operatively. On further follow-up, the histopathology of the resected specimen showed pT3N1Mx tumor and adjuvant chemotherapy with eight cycles of XELOX was given as recommended by the treating oncologist. His loop ileostomy was revered 12 weeks postoperatively without complications. On 1 year follow-up, the patient was doing well and free of the disease based on the recommend surveillance.
DISCUSSION
There are two main factors of most importance in evaluating a patient with rectal cancer and pelvic kidney. First, the anatomical consideration of the ectopic kidney where it has a highly variable blood supply as described by Dretler et al. [4] In 33 patients, 17 had single artery arising at or just distal to the bifurcation of the aorta, where 12 patient has dual blood supply one from the bifurcation and the other from the common iliac artery, and only 3 had triple blood supply (bifurcation, iliac and hypogastric) and 1 patient only with 4 blood supplying vessels with most of the time the blood vessel enters the kidney anteriorly. However, it has a less variable venous drainage. It is reported to drain mostly to the common iliac and/or distal vena cava vein. This consideration has a great value to properly plan the surgical steps and take the necessary precaution to prevent complication [2]. This could be achieved by CT scan or angiographic imaging to evaluate the vascular anomaly [5]. Based on the experience of the surgeon and the radiological imaging, it is crucial to put in mind the approach of surgery, either robotic, laparoscopy or open in regard to the safety, ease of accessibility and surgeon experience [2, 6].
The second factor is the need for radiotherapy in locally advanced disease, as it is evident that adding neoadjuvant radiotherapy for those patients has a great impact in controlling local recurrence. In one study, the rates of local recurrence at 2 years were 2.4% in the group assigned to the neoadjuvant radiotherapy with surgery and 8.2% in the group assigned to surgery alone [7]. For this reason, a multi-disciplinary team (MDT) discussion and patient involvement in making the decision of the available options is paramount.
Due to the extreme rarity of this condition, the literature lacks the guidelines for the most suitable management. If a patient has the coexistence of locally advanced rectal cancer and pelvic kidney, there are three described options. First, to proceed with nephrectomy if the preoperative investigations showed a nonfunctioning kidney to avoid complication such as acute and chronic nephritis, malignant and benign hypertension [1, 8]. Second, auto-transplant the kidney to a higher location away from the intended irradiated field; however, this technique is surgically difficult due to short ureter and vascular anomaly, and radiation effect is still a risk [1, 9]. The third option is the omission of radiotherapy with full explanation to the patient the risk of local recurrence and the need for close follow-up.
CONCLUSION
The coexistence of rectal cancer with ectopic kidney is a rare challenging scenario. Preoperative imaging and surgical planning are crucial to prevent inadvertent complication. Until now, there is no clear consensus regarding the optimal management option. For this reason, involvement of a MDT meeting and the patient understanding of the complication for the surgical option are important in making the decision. The literature needs more reported cases with long-term follow-up to increase the knowledge in our understanding of this disease entity.
CONFLICT OF INTEREST STATEMENT
The author declares no conflict of interest in this article.
FUNDING
None.
ETHICAL APPROVAL
No ethical approval needed as per IRB.
References
Siegel RL, Miller KD, Goding Sauer A, Fedewa SA, Butterly LF, Anderson JC, et al.

{kind=link}
{kind=link}
{kind=link}
{kind=link}