





Abstract
Fibroadenomas are benign breast tumors with a rare incidence of malignant transformation. Carcinoma arising within fibroadenomas typically occurs in women above the age of 40. We present a case of a young patient with microinvasive carcinoma arising within a biopsy-proven fibroadenoma, highlighting the possibility of carcinoma arising within fibroadenomas in young patients and the importance of vigilant surveillance even after a benign biopsy. In younger patients, new suspicious changes in benign lesions should be investigated. If prior core needle biopsy was performed, excision biopsy should be considered as the malignancy may be small and may be missed on needle biopsy.
INTRODUCTION
Fibroadenomas are benign fibroepithelial tumors and are the most common solid breast mass in women. Carcinoma arising within a fibroadenoma is very rare and typically occurs in women above the age of 40. We report a case of lobular carcinoma in situ with microinvasive carcinoma arising within a biopsy-proven fibroadenoma in a young patient.
CASE REPORT
A 26-year-old female presented with a longstanding palpable fibroadenoma in the left breast. She was first investigated with ultrasound imaging showing a lobulated 2.4 × 2.5 × 1.4 cm hypoechoic lesion with well-defined margins (Fig. 1). She underwent core needle biopsy of the lesion which was histologically proven to be a fibroadenoma. There was no evidence of malignancy. She was later discharged and presented 6 years later with a history of recent enlargement of the left breast lump. Ultrasound imaging now showed increase in the size of the left breast fibroadenoma to 3.2 × 2.7 × 1.6 cm and development of an irregular outline (Fig. 2). Because of increasing size of the lesion and new indeterminate features, excision biopsy was advised. Post-excision histology revealed a 5-mm focus of classic lobular carcinoma in situ (LCIS) with a 0.6-mm area of microinvasive carcinoma within the fibroadenoma (Figs 3–6). The carcinoma was estrogen and progesterone receptor positive and Her2 negative. Atypical ductal hyperplasia was seen in the breast tissue adjoining the fibroadenoma. After presentation at our multidisciplinary tumor board, sentinel lymph node biopsy for staging of the invasive carcinoma, radiotherapy and endocrine therapy for risk and recurrence reduction, as well as genetic testing in view of her young age was discussed with the patient. Because of the small size of the invasive carcinoma, potential cost and morbidity associated with sentinel lymph node biopsy, no further surgery was performed. The patient was agreeable to proceed with radiotherapy and endocrine therapy but requested to defer genetic testing.
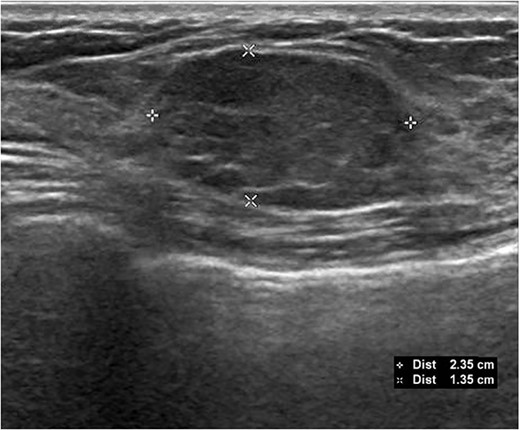
Initial ultrasound demonstrating the left breast mass measuring 2.4 × 2.5 × 1.4 cm. Core needle biopsy of this mass showed benign fibroadenoma with no malignancy.
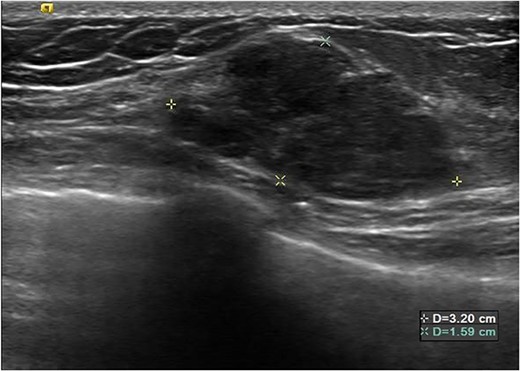
Subsequent ultrasound demonstrating increase in size of the left breast mass now measuring 3.2 × 2.7 × 1.6 cm. There was also new development of irregular margins, giving an indeterminate appearance.
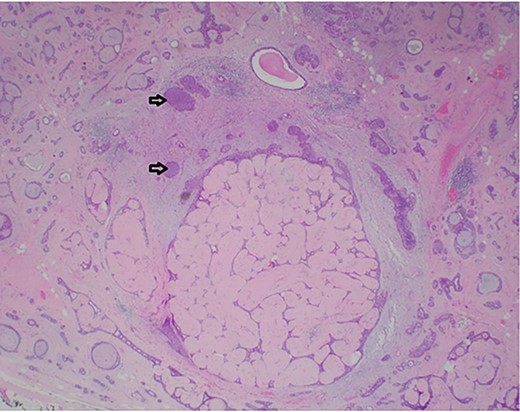
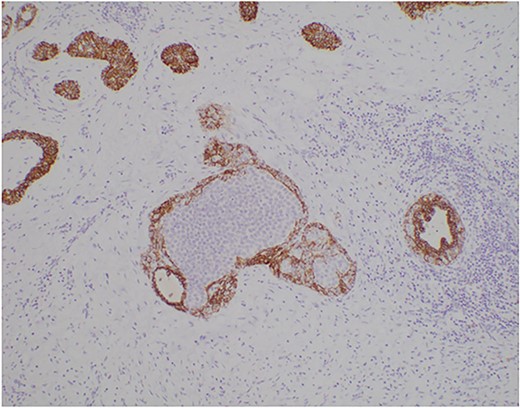
Photomicrograph showing a few ducts within the fibroadenoma expanded by a monotonous epithelial proliferation of classic lobular carcinoma in situ (arrows). (HE, ×20).
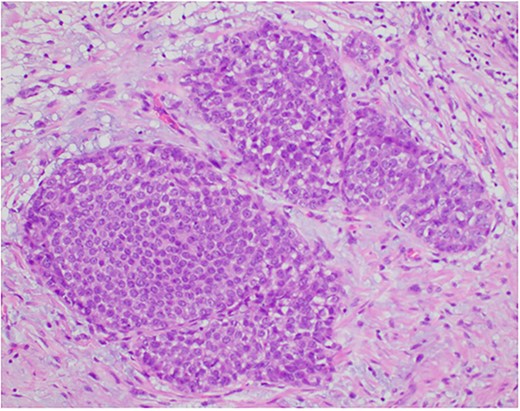
Photomicrograph showing the expanded ducts by classic lobular carcinoma in situ. (HE, ×200).
Photomicrograph of the classic lobular carcinoma in situ showing negative E-cadherin membranous staining. (E-cadherin, ×100).
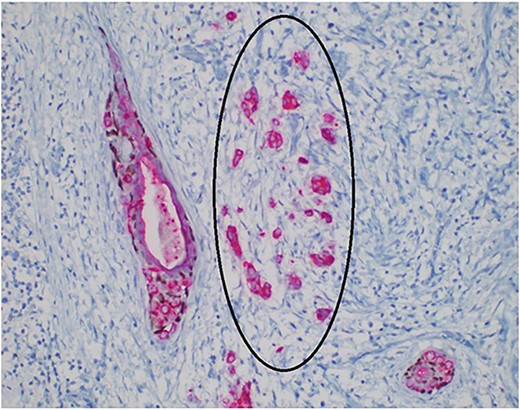
Photomicrograph showing a focus of microinvasive carcinoma (circle). (AE1/AE3/p63, ×400).
DISCUSSION
Fibroadenomas are benign fibroepithelial tumors most commonly found in women before 35 years of age with an estimated 10% incidence rate among females worldwide. Most fibroadenomas are clinically palpable as a mobile solid lump with rubbery consistency and regular borders, and further evaluation can be done using ultrasound, mammogram and core needle biopsy if indicated [1].
Carcinoma is diagnosed as arising within a fibroadenoma if: (i) The carcinoma is entirely encased within the fibroadenoma or (ii) if the carcinoma is only focally involved with the adjacent breast tissue [2]. The reported mean ages of patients with carcinoma in fibroadenoma are between 42 and 44 years of age, roughly 20 years after the peak age of occurrence [3–5]. The incidence of carcinoma arising within fibroadenoma is rare, ranging between 0.002 and 0.125% [6–8]. To date, <130 cases have been reported in the worldwide literature [4, 9–12]. Carcinoma in situ (both ductal and lobular) is the commonest type of malignancy [12]. Invasive carcinoma is rare, even more so for lobular carcinomas which make up 3.4% of malignancies in fibroadenomas [8, 9, 13]. Microinvasive carcinoma, defined by the latest Tumour, Node, Metastasis (TNM) classification as invasive carcinoma ‘with no invasive focus more than 1mm in greatest dimension’, is most frequently seen in association with high-grade ductal carcinoma in situ (DCIS), but also occurs in LCIS [14]. There has only been one reported case of microinvasive lobular carcinoma within a fibroadenoma described in a 51-year-old lady with no previous breast biopsy [15].
We present an unusual case of microinvasive carcinoma associated with classic lobular carcinoma in situ within a previously biopsied fibroadenoma in a young patient. Although she had imaging and core needle biopsy proving the mass to be a fibroadenoma with no evidence of malignancy, microinvasive carcinoma was eventually diagnosed after excision was performed due to recent significant increase in size and development of indeterminate features on sonography. This demonstrates the importance of vigilance during surveillance of patients with fibroadenomas as carcinoma can develop in young patients even with previously biopsy-proven benign lesions. If prior core needle biopsy has been performed, excision biopsy should be considered in cases of significant enlargement or development of new suspicious features as the malignancy may be very small and potentially missed on core needle biopsy.
CONCLUSION
Carcinoma can arise within fibroadenomas in young patients, and it is important to exercise vigilance for new suspicious changes in benign breast lesions. Excision biopsy should be considered in patients who had previous benign findings on core needle biopsy to avoid missing a malignancy.
PATIENT CONSENT
Consent was obtained from the patient who agreed with the publication of the case report.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
FUNDING
None.
DATA AVAILABILITY
All data available in main manuscript.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}