





Abstract
We present a case of a 30-year-old primigravida, at 38-week gestation, who had a posterior classical uterine incision due to a huge anterior wall leiomyoma associated with uterine torsion and breech presentation. The rarity of this type of uterine incision, the size of the uterine myoma and the uterine torsion prompted this case report.
During caesarean section, the diagnoses of uterine torsion and a huge anterior wall leiomyoma were made. She had safe delivery of the fetus through a posterior classical caesarean section. The patient had an uneventful post-operative period and was discharged home with her baby on the fourth post-operative day.
INTRODUCTION
Uterine torsion, defined as rotation of the gravid uterus >45 degrees, is a rare pathologic obstetric condition [1]. It can range from 60 to 720 degrees. Although, gravid uterus rotation <45 degrees is a common finding in the third trimester of pregnancy due to the increased uterine size and the presence of the rectosigmoid colon. Dextrorotation of the gravid uterus occurs more frequently than levorotation.
Although the exact aetiology is not known, uterine torsion has been reported in women with normal and abnormal pelvic anatomy such as uterine myomas, congenital uterine anomalies (bicornuate uterus and uterus didelphys), pelvic adhesion, ovarian cyst and abnormalities of the spine and pelvis and in the presence of fetal anomalies and malpresentation.
Uterine torsion may be asymptomatic or may present as failure to progress in labour, obstructed labour, intestinal obstruction, urinary complaints, abdominal pain, uterine hypertonus, vaginal bleeding and maternal shock [2]. The diagnosis is usually made incidentally at the time of caesarean delivery, and management is often derotation of the gravid uterus followed by lower segment transverse incision on the anterior uterine wall [1–4].
Classical uterine incision may be considered in situations in which access to the lower uterine segment is difficult as in the index patient. We present a case of uterine torsion of a myomatous uterus at term in which the fetus in breech presentation was delivered through a deliberate posterior classical hysterotomy.
CASE REPORT
A 30-year-old primigravida booked for antenatal care at 9-week gestational age. Her booking parameters were all normal. Pelvic ultrasonography showed a single intrauterine live fetus at 9 weeks and a solitary right lateral wall myoma measuring 17.4 cm × 11.2 cm. Her antenatal period was essentially uneventful. During her visit at 36 weeks, her abdomen was asymmetrically distended with increased prominence of the right half of the abdomen. Obstetric examination revealed a live fetus in oblique lie and breech presentation. Obstetric scan done confirmed a live fetus in breech presentation and a large myoma and tortuous dilated vessels on the lower myometrium on Doppler flow study.
She was counselled and scheduled for an elective caesarean section at 38-week gestation due to breech presentation in a primigravida with coexisting leiomyoma. Her preoperative investigations were normal.
At surgery, she was diagnosed with uterine torsion (120-degree dextrorotation) due to the right position of the left round ligament, fallopian tube and ovary. The torsion was corrected and a huge (about 40 cm × 40 cm) myoma was observed to occupy the entire anterior wall of the gravid uterus (Fig. 1a). There was no obvious uterine anomaly and the fallopian tubes and ovaries were grossly normal. The spinal anaesthesia was converted to a general anaesthesia with endotracheal intubation. The subumbilical skin incision was extended cephalad, and the gravid uterus and leiomyoma were exteriorized before a deliberate midline vertical incision was made on the posterior wall of the uterus and a healthy male baby was delivered by breech extraction. After delivery of the baby, she was given intravenous carbetocin 100 μg and tranexamic acid 1 g. The uterine incision was repaired in layers using 1–0 polyglactin suture and haemostasis was achieved as shown in Fig. 1b. The anterior abdominal wall incision was closed in layers with Nylon 2 suture to the rectus sheath. Her post-operative vital signs remained satisfactory, and she was discharged of fourth post-operative day.
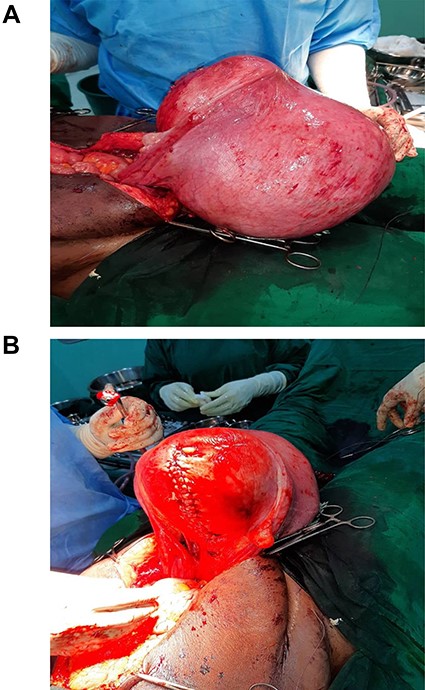
(A) Lateral view of myomatous uterus after delivery of the baby; (B) posterior view of myomatous uterus after repair of uterine incision.
DISCUSSION
This is a case of 120-degree torsion of a myomatous uterus at term with fetus in breech presentation that was delivered through a posterior classical hysterotomy. Even though the uterine torsion was reducible, the anterior uterine wall was completely inaccessible for hysterotomy due to the myoma. After derotation and exteriorization of the myomatous gravid uterus, a live male baby was safely delivered through the posterior classical caesarean section.
Classical uterine incision albeit a rare type of incision is associated with more intraoperative blood loss [5, 6, 7]; however, rapid repair of the uterine incision and judicious use of oxytocics minimized intraoperative blood loss.
In the case presented, the myomatous gravid uterus was associated with breech presentation and uterine torsion. Safe delivery of the mother and baby was achieved.
CONCLUSION
The use of classical uterine incision is rare but may be a life-saving procedure.
ACKNOWLEDGEMENT
The authors acknowledge the support of the Neonatologist, Nurses and staff members of the Modular Theatre, Lagos University Teaching Hospital Lagos.
CONFLICT OF INTEREST STATEMENT
None declared.
ETHICAL APPROVAL
Ethical approval was obtained from the Health Research Ethics Committee (HREC) of Lagos University Teaching Hospital.
CONSENT
A written informed consent was obtained from the patient for the manuscript.
GUARANTOR
I, Dr Aloy Okechukwu Ugwu will serve as guarantor for this case report.

{kind=link}