





Abstract
Small bowel rupture in blunt force trauma usually results from high-velocity and high-energy forces. The occurrence of this following collision in sport is a rare event that requires urgent surgical intervention. This is the case of a 27-year-old male who sustained a jejunal rupture following a collision during a game of soccer.
INTRODUCTION
Small bowel perforation from blunt force trauma is an infrequent occurrence. Small bowel injury occurs in 1.1% of blunt trauma, and of this, 0.3% are perforated [1]. This is usually a result of high-energy events such as motor vehicle accidents or falls from significant height. Serious hollow viscous injury from person to person contact in sport is a rarely reported incident.
CASE
A 27-year-old male presented to the emergency department shortly after an injury at a soccer game. The patient jumped to head the ball and received a knee into his abdomen. This was followed by immediate abdominal pain, though he was able to ambulate after the injury. A single episode of vomiting and development of left shoulder tip pain prompted his presentation to hospital. He had no significant past medical history. He presented with a heart rate of 75 bpm, a blood pressure of 134/81 mmHg, a respiratory rate of 24 breaths per minute and a temperature of 36.2°C. He had a tender abdomen with the point of maximal tenderness in the left upper quadrant with guarding and focal peritonism. His haemoglobin was 151 g/L, white cell count was 15.33 × 109/L with neutrophils of 13.03 × 109/L. His creatinine was 101 μm/L on presentation, and his liver function tests were unremarkable.
A chest X-ray did not show obvious pneumoperitoneum and a computed tomography scan demonstrated free gas in the abdomen with no solid organ injury (Figs 1 and 2). The patient was taken to theatre for a laparotomy and a 2 cm jejunal perforation was found on the mesenteric border, 10 cm from the duodenal–jejunal flexure. No other injuries were identified. A primary two-layer repair of the jejunum was performed with 4–0 polydioxanone suture. His postoperative recovery was unremarkable and was discharged after opening his bowels and tolerating oral intake at postoperative day 6.
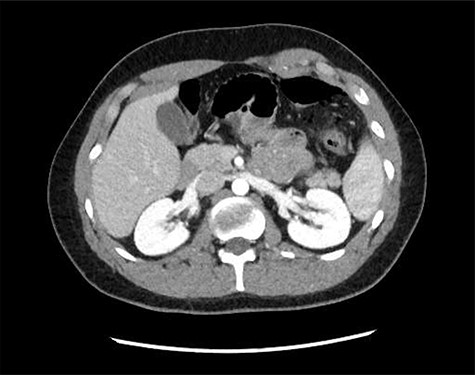
Axial computed tomography image demonstrating mesenteric stranding and free gas locules.

Coronal computed tomography image demonstrating free air.
DISCUSSION
This is a report on the case of a jejunal perforation following low-energy blunt trauma in sport. This is a rare injury in contact sports and is more commonly seen in high-velocity blunt force trauma. A review of 136 sports-related abdominal injuries in Skaraborg County in Sweden reported only three cases of small bowel injury [2]. A total of 12 cases of jejunal injury from sports have been reported in the literature globally, two of these have been from soccer [3]. Other sports involved include ice hockey, American football, cycling and rugby. A case of duodenal injury from a similar mechanism in our case has been reported on [4].
The proposed mechanism of injury has been from a combination of compression and shearing of the hollow viscus at the time of contact [5]. The two contacting surfaces are thought to be the anterior abdominal wall and the spine with the bowel between. Other possible mechanisms include a sudden increase in intraluminal pressure or a tangential tear along relatively fixed portions of the bowel [6]. Fixed areas of bowel such as the duodenum, terminal ileum and proximal jejunum are more susceptible. It is a difficult injury for on field medical teams to detect due to its relative rarity and lack of external signs at the time of injury.
Diagnosis is based on clinical suspicion about the degree of pain and examination findings and confirmed with radiological findings. Progressive abdominal pain with signs of peritoneal irritation raises clinical suspicion. Biochemical and frank radiological findings may become more marked as the time from injury progresses. Delayed diagnosis in blunt force trauma is associated with increased mortality and morbidity [7]. Prompt diagnosis and treatment is required to control the intra-abdominal sepsis.
CONCLUSION
Jejunal rupture relating from sports-related contact is a rare incident. Clinical suspicion can be confirmed with radiological investigations and prompt surgical intervention is required.

{kind=link}
{kind=link}