





Abstract
Tumors of the upper urinary tract are discovered, either by clinical symptomatology or as part of the evaluation of a bladder tumor. Hypercalcemia is one of the most common paraneoplastic syndromes and an exceptional complication of urothelial carcinoma of the upper tract. Several physiopathological mechanisms have been proposed to explain this rare and serious complication. Hypercalcemia is often correlated with tumors with a poor prognosis.
INTRODUCTION
Bladder cancer is one of the most common cancers; it is fifth in order of frequency and responsible for 3% of cancer deaths, including 75% in humans.
It is the second urological cancer after prostate cancer. Most urothelial tumors appear after the age of 60. In all, 2–4% of patients with bladder tumors develop an upper urinary tract tumor metachronous or synchronous [1], but some studies report higher percentages as high as 20%.
Our work aims to report the case of a patient who developed major hypercalcemia in a paraneoplastic syndrome resolved after removal of the tumor mass from the upper excretory tract.
OBSERVATION
This is the case of a 52-year-old patient, a chronic smoker for 32 Unit-Package-Year. The patient had no disease or hypercalcemic treatment. He presented to the consultation with intermittent low back pain evolving for 2 years in a context of apyrexia, associated with episodes of total clotting hematuria. The clinical examination revealed a patient in good general condition, with slightly discolored mucous membranes with the presence of pain on palpation in the left flank and lumbar contact.
Laboratory assessment showed anemia at Hb: 7 g/dl with hyperleukocytosis 44 600/mm3 predominantly neutrophilic.
Ultrasound showed a solid-cystic left renal process, the right kidney well differentiated with thickening of the bladder wall.
Abdomino-pelvic computed tomography scan revealed an enlarged left kidney, a lump in the lumbar ureter, and irregular thickening of the bladder wall. (Figs 1 and 2).
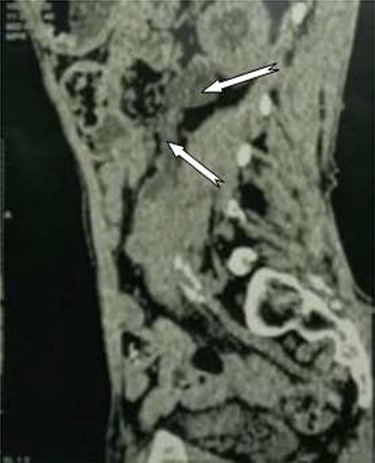
Tumor process at the expense of the kidney and the left urethra.

Irregular thickening of the bladder wall.
The patient underwent transurethral resection with several pedunculated tumors in the lumen of the bladder, the histopathological study of which was in favor of a high-grade urothelial carcinoma, infiltrating the chorion with a non-infiltrated detrusor muscle.
During hospitalization, the patient developed hypercalcemia at 155 mg/L which required an extra-renal purification session. Given the persistence of hypercalcemia and despite symptomatic measures, the patient was referred to the operating room for a right nephroureterectomy and cystoprostatectomy with dissection of the extensive bilateral Ilio-obturator lymph nodes and left cutaneous ureterostomy (Fig. 3).

Specimen of right radical nephro-ureterectomy and cystectomy.
A histopathological examination of the tumor mass revealed a urothelial carcinoma of the kidney infiltrating the parenchyma and respecting the renal capsule and the adrenal gland. At the level of the ureter, a high-grade urothelial carcinoma observed infiltrating the chorion. We found the same histological appearance in the bladder but the detrusor was not infiltrated.
The postoperative follow-up was simple, with normalization of the serum calcium level on the first postoperative day and resumption of transit on the third postoperative day. The patient was discharged on the tenth postoperative day.
DISCUSSION
Paraneoplastic syndrome is a clinical and biological manifestation that can complicate solid cancers, independent of its size, local or distant invasion. It is linked to the uncontrolled secretion by tumor cells of substances such as hormones, growth factors, cytokines, and tumor antigens.
Hypercalcemia most often accompanies cancer of the breast, prostate and lung. The mechanisms of hypercalcemia are varied:
Hypercalcemia due to the activation of osteoclasts by various substances produced by tumor cells: lymphotoxin, Interleukin 6 (IL-6), IL-1, parathormone-related protein (PTHrP) and hepatocyte growth factor (HGF)
Hypercalcemia results from the tumor secretion of hypercalcemic factors stimulating parathyroid receptors in the bones and kidneys, leading to diffuse bone resorption with decreased tubular reabsorption of phosphate and increased tubular reabsorption of calcium.
Ectopic hyperparathyroidism corresponding to the production of parathyroid hormone by a non-parathyroid tumor, a rare event reported in neuroendocrine tumors of the ovary, lungs, and thyroid.
The severity of hypercalcemia is related to metabolic disturbances leading to dehydration and subsequent acute renal failure. Hypercalcemia greater than 150 mg/L is a medical emergency because of the risk of coma with collapse and cardiac arrest. Management of life-threatening hypercalcemia consists of saline rehydration combined with slow infusion of bisphosphonate. Hemodialysis also helps to lower serum calcium and to control metabolic complications [2]. While clear cell renal tumors are associated with hypercalcemia in 20% of cases, hypercalcemia is rare and atypical in urothelial tumors. The mechanism of hypercalcemia is humoral by the production of PTHrP, which remains the most widespread theory. More recently, other mechanisms have been discovered explaining that urothelial tumors secrete the colony-stimulating granulocytic factor (G-CSF) responsible for the hyperleukocytosis associated with hypercalcemia [3]. This substance, which stimulates the proliferation of granulocytes, promotes tumor growth and aggressiveness which begins to produce more PTHrP [3].
All cases of hypercalcemia reported in the literature are corrected after tumor ablation, although the agent responsible for this event has not been identified. However, hypercalcemia remains a factor of poor prognosis in urothelial tumors [4].
CONCLUSION
Paraneoplastic syndrome is a clinical and biological manifestation associated with cancer, hypercalcemia is rarely found in urothelial tumor. The exact mechanism remains unknown; however, its presence is a marker of poor prognosis.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
Note.
CONSENT TO PUBLICATION
The consent to publish this information was obtained from study participants. We confirm that written proof of consent to publish study participants are available when requested and at any time.
AVAILABILITY OF DATA AND MATERIAL
The datasets in this article are available in the repository of the urology database, Chu Ibn-Rochd Casablanca, upon request, from the corresponding author.
AUTHOR CONTRIBUTIONS
I.J., A.M., E.W. and M.G. analyzed and performed the literature research; M.D., A.D. and R.A. performed the examination and performed the scientific validation of the manuscript. I.J. was the major contributor to the writing of the manuscript. All authors read and approved the manuscript.

{kind=link}
{kind=link}
{kind=link}