





Abstract
Complete colonic duplication is rare and frequently asymptomatic. We present an interesting case of tubular colonic duplication with associated uterine didelphys and a longitudinal sagittal septum in the bladder, noted incidentally on cross-sectional imaging. The patient was later diagnosed with ulcerative colitis affecting the duplicated colon and is currently in remission following medical therapy.
INTRODUCTION
Gastrointestinal duplication is a rare clinical entity, which can affect any part of the alimentary tract. Between 67 and 80% of gastrointestinal, duplications present before the age of 2 years [1]. Lesions can be cystic or tubular in nature and affect the ileum in ~60% of cases [2]. Colonic duplications are comparatively rare and can be communicative or non-communicative in nature, with respect to adjacent bowel. We present an interesting case of tubular colonic duplication with didelphys and a longitudinal sagittal septum in the bladder, noted incidentally on cross-sectional imaging in an adult patient.
CASE REPORT
A 28-year-old woman presented to the emergency department with a 1-week history of abdominal pain, bloating and constipation. A computed tomography (CT) scan was performed, which demonstrated distension and a lead pipe appearance of the right colon suggesting a mild colitis (Fig. 1). The CT scan also demonstrated a duplicated segment of colon with a blind ending proximal limb (Figs 1 and 2), uterine didelphys (Fig. 2) and a duplicated bladder (Fig. 3). A subsequent magnetic resonance imaging scan demonstrated an 11 cm segment of thickened bowel with mucosal ulceration and surrounding hyperaemia confined to the duplicated colon. Sigmoidoscopy was performed and histology from the duplicated descending colon demonstrated mild active chronic colitis with crypt inflammation and associated abscesses without granuloma formation. The native colon had an unremarkable appearance. The patient was started on mesalazine and has had no further complaints of abdominal pain or bloating.

Coronal CT scan demonstrating native and duplicated tubular colon (indicated by blue arrows).
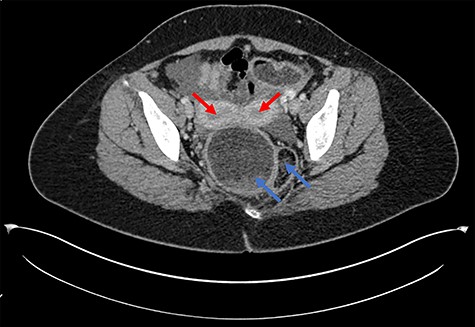
Axial CT scan demonstrating uterine didelphys (red arrows) and duplicated rectum (blue arrows).
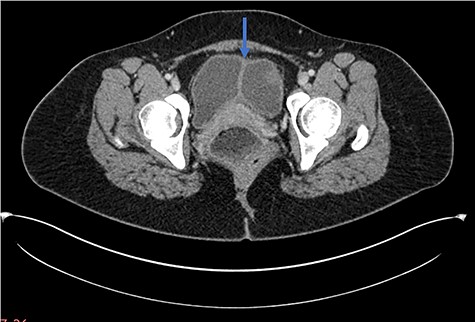
Axial CT scan demonstrating longitudinal sagittal septum giving rise to a duplicated bladder appearance.
DISCUSSION
Colonic duplication may be related to incomplete recanalization of the bowel lumen during the first trimester; communication between native and duplicated bowel may or may not be present [3]. A descriptive classification system has been described for colonic duplication, although it remains a rare clinical entity [4]. A recent review of colonic duplication cases found the most common presenting complaint to be abdominal pain with the transverse colon most commonly affected [1].
Uterine didelphys results from incomplete Mullerian duct fusion and has varying reproductive outcomes. The incidence of Mullerian duct abnormalities ranges from 0.5 to 5%, with didelphic uteri representing 11% of uterine malformations [5]. The incidence is comparable between infertile and fertile cohorts [6], although the term delivery rate for patients with uterine didelphys is only 45% [7]. Duplication of the bladder is another rare clinical entity, arising from a complete sagittal septum of the bladder. Cases have been reported in the literature, although little is understood about the underlying aetiology [8, 9].
We present an interesting case of multiple, rare congenital anomalies in a single adult patient incidentally found on cross-sectional imaging.
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts of interest to declare in relation to the current work.
FUNDING
No funding received.

{kind=link}
{kind=link}
{kind=link}