





Abstract
Intussusception in adults is, especially with ulcerative colitis (UC), rare and only described in a few cases. Most adult patients with intussusception develop abdominal pain or other symptoms of bowel obstruction. This case describes an 18-year-old male with UC who treated with 5-aminosalycilicacid and underwent annual screening colonoscopies. Two attempts revealed that it was impossible to achieve total surveillance through the colonoscopy because multiple polyps were preventing the colonoscope from traversing the entire colon. Therefore, CT scan was performed and colonic intussusception was discovered incidentally, and the patient underwent elective laparoscopic total colectomy. To the best of our knowledge, this is the first reported case of asymptomatic intussusception in the adult patient with UC. When total surveillance colonoscopy fails to yield results, a CT may be advisable to pick up such an asymptomatic intussusception.
INTRODUCTION
Intussusception, a telescoping of a segment of bowel into the lumen of an adjace0nt segment, is a rare cause of acute abdomen in adults (1). Intussusception is particularly rare with ulcerative colitis (UC), and only five cases of intussusception in patients with UC have been reported thus far (2–6). The clinical presentation of adult intussusception is variable but generally marked by abdominal pain or signs of bowel obstruction (1). All the previous reported cases of intussusception with UC also had abdominal pain as the initial symptom. We describe a patient with UC who developed asymptomatic intussusception.
CASE REPORT
An 18-year-old man came to our hospital having initially sought treatment at the age of 16 for bloody stool. Colonoscopy revealed multiple inflammatory polyps less than 1 cm throughout the colon and the patient was diagnosed with UC by biopsy. He was initially treated with tacrolims to induce remission and was subsequently administered 5-aminosalycilic acid orally for maintenance of remission. A year later, surveillance colonoscopy failed completely because polyps in the transverse colon closed the lumen. Having no abdominal pain or the other symptoms, and no abnormalities in laboratory values, he did not undergo detailed examination at that time. Thereafter, surveillance colonoscopy the following year also failed to show the total colon, (Fig. 1A and B) a computed tomography (CT) was performed. The CT revealed elongated mass lesion in the area of the transverse colon, and the patient was diagnosed with colonic intussusception (Fig. 1C). Because he still had no symptoms, nor laboratory abnormalities, we performed to endoscopic enema reduction. Enema reduction had failed because air had passed through the lead-point of intussusception in transverse colon. Accordingly, the patient underwent elective laparoscopic total colectomy for treatment of the intussusception with UC. The operative finding revealed inversion of the transverse colon into the distal transverse colon. Histology showed widespread inflammatory polyps with no evidence of neoplasia (Fig. 2A and B). The patient’s postoperative course was uneventful, and he was discharged 28 days after surgery.
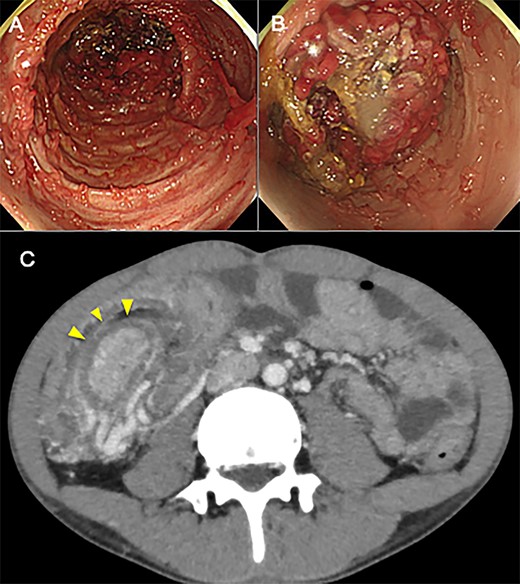
(A, B) Colonoscopy before total colectomy shows multiple polypoid structure throughout the colon, especially in the transverse colon in which colon was in invagination. (C) CT before total colectomy shows an elongated mass lesion in the transverse colon. An oval mass (arrowhead) represents intussuscepted bowel wall, surrounded by mesenteric fat and vessels of the intussuscipiens.
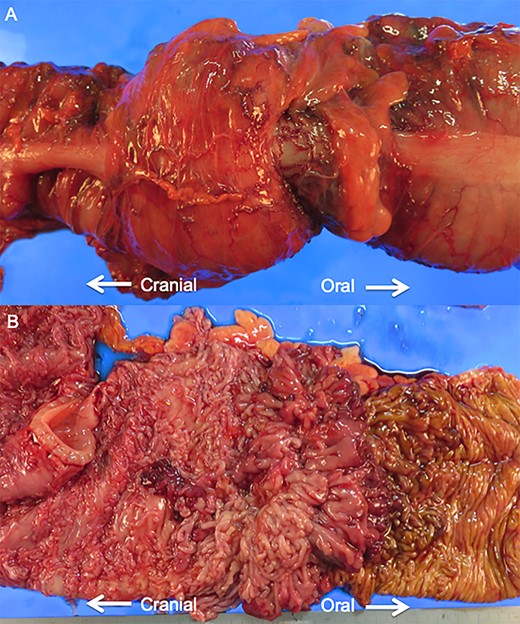
(A) Gross feature of surgical resection specimen. The proximal transverse colon has invaginated into the distal transverse colon. (B) Opened surgical specimen. Numerous inflammatory polyps spread throughout the entire colon.
DISCUSSION
To date, only five cases of intussusception with UC in adults have been reported (Table 1). Most intussusceptions in adults are caused by neoplastic lesions, especially colonic intussusception, in which a tumor-related lesion serves as the lead-point in more than 75% of cases (7). However, none of the previously reported cases of intussusception with UC were associated with tumor-related lead-point; this was also true in our case (2–6). Of the five cases, structural lead-point was inflammatory polyps in three cases, Cytomegalovirus infection in one case, and appendicitis in the last case. One possible reason that patients with UC do not have tumor-related lead point is that UC patients undergo annual colonoscopies. Frequent colonoscopies may prevent tumor from growing large enough to cause intussusception.
Review of reported cases of adult intussusception with UC
| Author | Year | Age | Gender | Location | Etiology | Symptom | Treatment |
|---|---|---|---|---|---|---|---|
| Forde et al. (1) | 1978 | 22 | Male | Transverse colon | Inflammatory polyps | Abdominal pain | Surgical resection |
| Maldonado et al. (2) | 2004 | 27 | Male | Splenic flexure | Inflammatory polyps | Abdominal pain | Surgical resection |
| Esaki et al. (3) | 2009 | 27 | Male | Hepatic flexure | Inflammatory polyps | Abdominal pain | Enema reduction |
| Coghlan et al. (4) | 2010 | 35 | Female | Transverse colon | CMV infection | Abdominal pain | Conservative medical approach |
| Burchard et al. (5) | 2018 | 39 | Female | Appendix | Appendicitis | Abdominal pain | Surgical resection |
| Current case | 2020 | 18 | Male | Transverse colon | Inflammatory polyps | None | Surgical resection |
In contrast to previous reports of intussusception with UC, our patient had no symptoms. Although patients with intussusception has historically presented with a bowel obstruction-like syndrome, increasing cases of transient or asymptomatic intussusception are being identified as imaging techniques become more sophisticated. Transient or asymptomatic intussusception account for ~20% of all cases of intussuseption in adults, and our case seems to be an incidental radiologic finding (1). The reason that our patient remained asymptomatic is presumed that inflammatory polyps were relatively small compared to previously reported cases (2–4). This situation allowed luminal traversability, and CT revealed the intussusception before any traditional symptoms occurred.
CT is the most useful examination for diagnosing intussusception, as it provides an accurate diagnosis in 78% of patients (8). In our case, surveillance colonoscopy failed to traverse entire colon, and CT for detailed examination detected colonic intussusception incidentally. These results suggest that CT may be useful when the bowel lumen is not traversed by colonoscopy in patients with UC, even when such patients have no abdominal symptoms. Failure of total colonoscopy can be one reason for suspecting asymptomatic intussusception, as in our case.
In conclusion, adult intussusception with UC dose occurs without any symptoms, and failure of surveillance total colonoscopy may be one reason to suspect intussusception, despite the lack of symptoms, and in such case, a CT scan is useful for diagnosis.
CONFLICT OF INTEREST STATEMENT
None Declared.
ACKNOWLEDGEMENTS
The authors thank Makoto Kodama for his help in pathological diagnosis. We also thank Angela Morben, Doctors of Veterinary Medicine, Editor in the Life Sciences, from Edanz Group (www.edanzediting.com/ac), and Shari J. Berman, from Japan Language Forum, for editing a draft of this manuscript.

{kind=link}
{kind=link}