





Abstract
Truncus arteriosus (TA) is a relatively uncommon cyanotic congenital cardiac anomaly accounting for 1.3% of all congenital cardiac malformations. TA associated with an ascending aortic aneurysm is an extremely rare congenital cardiovascular abnormality. A 15-year-old male presented with shortness of breath and cough for 2 weeks. Radiological examinations showed that the ascending aorta and main pulmonary arteries originate from a single truncus with ascending aortic aneurysm. TA has a poor prognosis if remain unrepaired and surgical intervention is necessary to avoid severe pulmonary vascular occlusive disease.
INTRODUCTION
Truncus arteriosus (TA) is a relatively uncommon cyanotic congenital cardiac anomaly that accounts for 1.3% of all congenital heart defects (CHD) and is characterized by a single arterial trunk originating from the heart, which in turn gives rise to the pulmonary artery, coronary arteries and systemic blood flow [1].Ascending aortic aneurysms are irreversible dilatations of the ascending aorta of >50% of normal diameter with an incidence of 4.5 per 100 000 of people [2]. TA associated with ascending aortic aneurysm is an extremely rare congenital cardiovascular abnormality. Here we report a case of a 15-year-old male presenting with an unusual combination of silent TA Type-II with a 7 cm ascending aortic aneurysm.
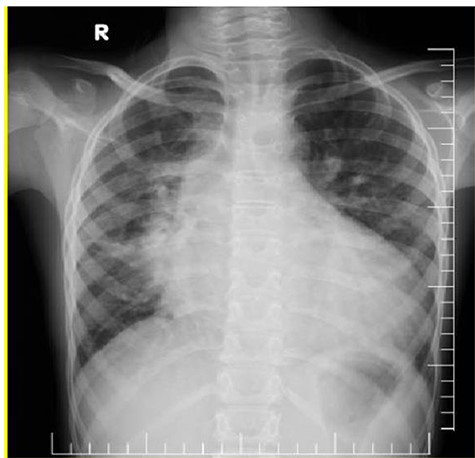
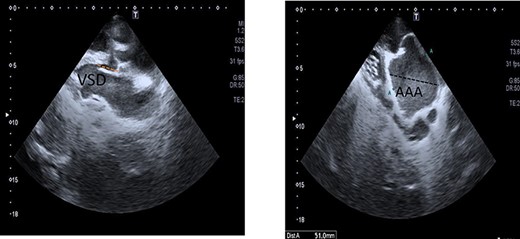
(A) Chest X-ray showed prominent pulmonary vascular marking, atelectasis in the right lung and cardiomegaly with a widening mediastinum. (B and C) Echocardiography: short-axis view revealed VSD (B) and long-axis view showed ascending aortic aneurysm (C).
CASE REPORT
A 15-year-old male presented to our hospital with a history of shortness of breath and cough for 2 months. The patient was one of five children with no family history of CHD. His growth had been normal and there was no history of recurrent or chronic illness during his life. On examination, his blood pressure was 120/70, SpO2 was 97%, digital clubbing was present, a parasternal heave was noted in the left second intercostal space and a systolic murmur was present. All his blood tests were normal. Electrocardiogram was normal and a chest radiograph showed prominent pulmonary vascular markings, atelectasis in the right lung and cardiomegaly with a widening of the mediastinum due to a large aortic shadow (Fig. 1).
Contrast thoracic CT showed the left main pulmonary artery (A: red arrow) and right main pulmonary artery (B: red arrow) originate from a single truncus. It was evaluated as compatible with the TA and combined with ascending aortic aneurysm (A and B: red arrows).
Echocardiography was done and a short-axis view revealed that the right and left pulmonary artery originate from common arterial trunk with no main pulmonary artery segment. The long-axis view showed a VSD and an ascending aortic aneurysm (Fig. 1B and C). Contrast chest computer tomography (CT) showed the ascending aorta and main pulmonary arteries originate from a single common trunk (Fig. 2A and B).
No other abnormal findings were found. The patient was stable and managed with furosemide and recommended to contact the hospital if he developed any clinical features of heart failure, pulmonary hypertension or infective endocarditis. The patient was advised to look internationally for surgical options as unfortunately such a complex repair is not available in Somalia.
DISCUSSION
Among congenital heart disease, TA is a relatively uncommon cyanotic congenital cardiac anomaly accounting for 1.3% of all CHD. TA is characterized by a single arterial trunk originating from the heart, which in turn gives rise to the pulmonary arteries, coronary arteries and systemic blood supply [1].
According to the Collett and Edward’s classification, TA is classified into four types according to the anatomical position of pulmonary arteries. The presenting case had a Type II TA due to a single common trunk with two pulmonary arteries arising from posterior portion of the aorta.
TA can be associated with cardiac and extracardiac malformations as well. Eroksuz and colleagues reported a case of TA with an intact ventricular septum. It is fascinating to recognize that the present case had TA combined with a VSD and an ascending aortic aneurysm [3].
TA usually presents with shortness of breath, tachypnea, poor feeding, cyanosis, signs of heart failure and failure to thrive within the first few weeks of life [4].
This case report illustrates a rare combination of late-presenting TA and ascending aortic aneurysm. Unrepaired TA can be associated with high morbidity and mortality without surgical intervention and the mortality rate can be up to 85% at 1 year of age depending on cardiac or extracardiac malformations [5]. We believe that this patient survived at birth because the pulmonary vascular resistance remained high and this prevented excessive pulmonary blood flow to cause pulmonary overcirculation.
Most cases of TA have a poor prognosis if remain unrepaired and surgical intervention is necessary to avoid severe pulmonary vascular occlusive disease. To our knowledge, his is the first case reported from Somali with this rare clinic association.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}