





Abstract
Our patient was a 59-year-old woman with past history of hysterectomy, bilateral salpingo-oophorectomy, regional lymphadenectomy and omentectomy performed for advanced ovarian cancer. She was experiencing abdominal pain over the past 2 days and visited our hospital owing to pain exacerbation. Contrast-enhanced computed tomography revealed free air around the liver, ascites and duodenal perforation; thus, emergent abdominal surgery was performed. The 5-mm duodenal perforation at the anterior wall of the duodenal bulb was sutured with absorbable thread. We used ligamentum teres hepatis (LTH) as a patch for the sutured site as the greater omentum could not be used. The postoperative course was uneventful, and she was discharged on postoperative Day 8. There were no complications 1 month after surgery. Although the greater omentum is conventionally used for upper gastrointestinal perforation, the LTH was a plausible alternative with good indication in our case.
INTRODUCTION
Ligamentum teres hepatis (LTH) is the umbilical vein remnant and can be found in the free edge of falciform ligament of the liver. Fry et al. [1] reported the first use of LTH for perforated peptic ulcer in 1978. Thereafter, limited similar case series of LTH use have been reported [2–5]. Although the use of LTH procedure has been previously reported, these surgical indications have never been reported. We herein describe duodenal perforation following omentectomy for ovarian cancer. To our knowledge, this is the first case with apparent surgical indication of LTH use for perforated duodenal ulcer.
CASE REPORT
Our patient was a 59-year-old woman with past history of hysterectomy, bilateral salpingo-oophorectomy, regional lymphadenectomy and omentectomy performed for advanced ovarian cancer 3 years prior. She was experiencing abdominal pain over the past 2 days and visited our hospital owing to pain exacerbation. Contrast-enhanced abdominal computed tomography showed free air with ascites around the liver and duodenum perforation (Fig. 1). Tenderness and muscular defense were found mainly in the upper abdomen. Her white blood cell count and C-reactive protein levels were 17 200/μl and 0.04 mg/dl, respectively. Our clinical diagnosis was duodenal perforation with peritonitis.
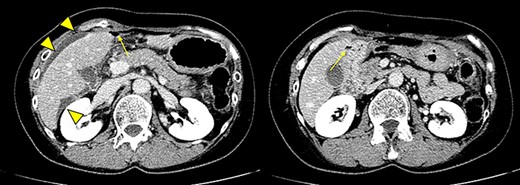
Contrast-enhanced abdominal computed tomography showing free air (arrow) and ascites (arrowhead) around the liver and duodenal perforation.
As the patient had a history of omentectomy and conventional repair, using the omentum was impossible; thus, we performed an emergent abdominal surgery using LTH, assuming intraabdominal severe adhesion following omentectomy and laparotomy, which is not generally suitable for laparoscopic surgery. A 5-mm perforation at the anterior wall of the duodenal bulb was observed (Fig. 2a). The perforated duodenum was sutured using 3–0 VICRYL® (Ethicon, Japan). LTH was used to protect the sutured duodenum (Fig. 2a to b) and fixed to the duodenum using 3–0 VICRYL® (Ethicon, Japan). The operative time was 74 min with a 6-ml blood loss.
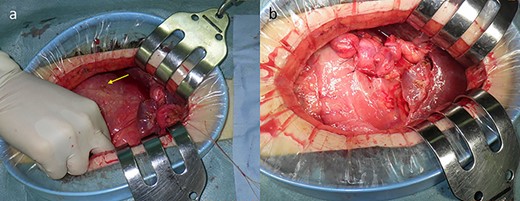
Intraoperative findings showing duodenal perforation (arrow) (a) and repair using LTH (b).
Postoperative course was uneventful; a proton pump inhibitor was administered orally, and the patient was discharged on postoperative day 8. Serum antibody examination for Helicobacter pylori was negative. The patient is being followed up by a gynecologist and has shown no apparent evidence of recurrent ovarian cancer or duodenal ulcer.
DISCUSSION
Surgical management for a perforated duodenal ulcer includes using an omental patch with or without primary closure of the perforation or omental plug. Graham first reported using the omentum for duodenal perforation; thus, the procedure has been recognized as the Graham patch technique [6]. Further, since the surgical management of a perforated peptic ulcer was first performed laparoscopically in 1990, the laparoscopic approach has been widely adopted to treat perforated duodenal ulcers [7]. In our institution, laparoscopic repair for upper gastrointestinal perforation is a standard approach.
LTH, including the falciform ligament, is rich in vessels like the greater omentum [8]. The efficacy of LTH for preventing hemorrhages from the gastroduodenal artery following pancreatoduodenectomy, besides perforated duodenal ulcers, has been reported [9]. As the ligament is located near the duodenum, using LTH to repair perforated duodenal ulcers is anatomically plausible.
Despite previous studies describing this alternative technique, clinical indications for LTH use remain unknown. In our patient, omentectomy was performed to treat ovarian cancer before surgery; therefore, using LTH for perforated duodenal ulcer repair was planned preoperatively. Despite a history of omentectomy and laparotomy, laparoscopy will be a feasible option in this case, as severe adhesion was not observed in our patient. Based on the successful postoperative course of our patient, laparoscopic treatment of peptic duodenal ulcers using LTH can be considered effective and appropriate for patients with past history of omentectomy.
ACKNOWLEDGEMENTS
We thank Editage for editing a draft of this manuscript.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}