





Abstract
This is an extremely rare presentation of multiple appendicoliths in one appendix. Multiple appendicoliths as well as appendicoliths larger than 5 mm have been implicated in severe appendicitis as well as perforation and gangrene of the appendix. There is no known correlation with appendicular malignancy. The controversy arises in the surgical management of asymptomatic patients. There is emerging evidence that justifies an elective appendicectomy in asymptomatic patients.
INTRODUCTION
We present an unusual case of acute appendicitis associated with multiple appendicoliths of considerable size. These were initially identified on computed tomography (CT) scan during the patient’s pre-operative workup for acute abdominal pain, and the appendicitis was managed emergently with a laparoscopic appendicectomy. The procedure was completed without incident, and examination of the appendix confirmed the radiological findings with four appendicoliths larger than 5 mm within the lumen. Appendicoliths are well described in the English literature as incidental findings on imaging and as obstructive causes of acute appendicitis. They have not been formally reported upon in larger numbers. Emerging research suggests a correlation between the number of appendicoliths found on CT imaging, their size and the likelihood of developing acute appendicitis, which raises interesting questions about the prognostic value of similar imaging findings and their possible implications for elective surgical management in asymptomatic patients.
CASE REPORT
A 66-year-old male patient who had undergone bilateral blepharoplasty 3 days earlier was referred to our acute care surgical service with a 24-hour history of increasing right lower quadrant pain accompanied by nausea, vomiting and anorexia. Clinically he was found to be afebrile with a soft abdomen and focal tenderness at McBurney’s point. Significant laboratory investigations revealed a leukocytosis of 13.0. A CT scan of the abdomen confirmed the diagnosis of appendicitis with an impacted appendicolith at the appendicular outlet and a number of additional appendicoliths distributed along the length of the appendicular lumen (Figs 1–2). The patient was surgically consented for a laparoscopic appendicectomy with intraoperative video recording. At laparoscopy an inflamed and focally necrotic appendix was located coiled over the cecum (Figs 3–4). The appendectomy was completed without complication, and the specimen longitudinally transected in the operating room prior to pathological submission. This revealed four appendicoliths within the lumen, all measuring over 5 mm at their smallest diameter (Fig. 5). Pathology confirmed acute suppurative appendicitis with transmural necrosis, with the appendicoliths described as faeculent in origin. The patient’s post-operative recovery was uneventful.

Sagittal view of the abdominal CT showing multiple appendicoliths within a dilated appendix (white arrows).
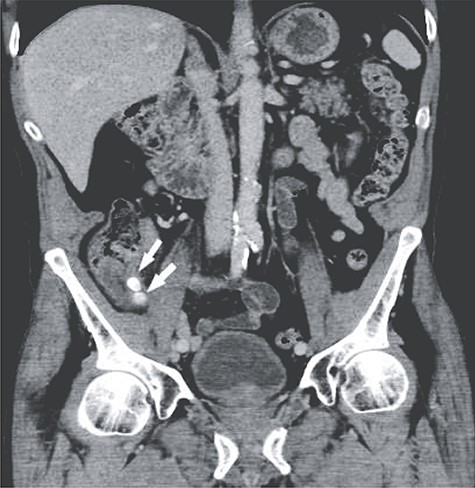
Coronal view showing two of the larger appendicoliths at the appendix base (white arrow).

Intraoperative picture demonstrating the inflamed and coiled appendix with signs of transmural necrosis.

Intraoperative picture demonstrating the inflamed and coiled appendix with signs of transmural necrosis.

The transected appendix with four easily identified appendicoliths (white arrow).
DISCUSSION
Appendicoliths are well described in the English literature as a common incidental finding on imaging and an important factor in the pathogenesis of acute appendicitis through luminal obstruction [1]. They are present in 18% of acute appendicitis [2]. The majority are faecal in origin with intestinal mucus, inorganic salts and calcium deposition contributing to their structural framework [3].
Migrating gallstones found in an acutely inflamed appendix have also been implicated in their epidemiology [4]. Appendicoliths are typically identified in young adults and the paediatric population [5] and are associated with a higher incidence of perforation and abscess formation [6]. Appendicoliths giving rise to recurrent appendicitis have rarely been described [7]. There has been no documented association between appendicoliths and appendicular malignancy. This case report is unusual given the number of appendicoliths present on imaging and confirmed visually at surgery. To our knowledge, this is the largest documented number of appendicoliths, in a single appendix reported in the English literature. All four of the primary appendicoliths were more than 5 mm in size, and the patient’s age is also atypical as appendicoliths are usually found in a younger surgical cohort.
The higher number of appendicoliths and their larger size are of particular interest given their prognostic implications. CT imaging preoperatively was conducted to prove a diagnosis of acute appendicitis. The controversy arises in incidentally discovered multiple appendicoliths on radiological imaging. There is currently no consensus as to the clinical implications of radiologically discovered incidental appendicoliths in asymptomatic patients.
There is emerging evidence that certain specific appendicolith features may have clearer clinical relevance. Khan et al. [8] in a cross-sectional study on 321 patients, demonstrated that CT findings of more than one appendicolith and an appendicolith diameter larger than 5 mm on CT were associated with a higher likelihood of concomitant acute appendicitis. Ishiyama et al. using multivariate analysis also found a positive relationship between appendicolith size greater than 5 mm and gangrenous appendicitis (OR of 3.0) [9]. It is conceivable that larger numbers of appendicoliths and larger-sized appendicoliths found on CT may increase the likelihood of acute appendicitis and that these findings may be significant enough to support a recommendation of an elective appendectomy in asymptomatic patients.
CONCLUSION
We believe this to be the first case report in the English literature of a clinical presentation with four appendicoliths in a single appendix. Further research into the relationship between the size and number of appendicoliths visualised radiologically will help ascertain appropriate clinical counselling and definitive surgical management in asymptomatic patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}