





Abstract
High pressure injection injuries to the hand should not be taken lightly as urgent surgical debridement is required to ensure favorable outcomes. Empiric antibiotic administration is recommended; however, few studies focus on the secondary infection risk associated with these high pressure injection injuries. We present a rare case of a patient presenting with carbapenem resistant Pseudomonas aeruginosa following a high pressure paint gun injury of the thumb. Urgent surgical debridement with administration of broad-spectrum antibiotic coverage for both gram-negative and gram-positive bacteria is recommended. The injection of foreign materials can cause extensive tissue damage and immunosuppression facilitating growth of opportunistic bacteria that are often rare in healthy adults. We advocate for obtaining cultures at initial debridement to optimize treatment in these unique and rare injection injuries. Concerns should be raised as carbapenem resistant bacteria become more prevalent in the community.
INTRODUCTION
High pressure injection devices such as paint or grease guns can cause penetration of the skin and damage to tissues beneath. Rare cases have shown foreign material traveling as far as the axilla and mediastinum [1]. The extent of injury is generally dependent on multiple variables, including the type of chemical, injection pressure, quantity of material, site of injection and time to presentation [2]. A high pressure injection injury is considered a surgical emergency and irrigation and debridement (I&D) is recommended within 6 h [3]. Despite aggressive treatment, amputation rates range from 22 to 48% [1].
Over 100 case reports of high pressure injection injuries have been described, however few studies focus on infection secondary to the injury [4]. Microbes that are native flora of the skin are the primary cause of soft tissue infection in trauma patients. The majority of these infections are caused by Staphylococcus aureus, beta-hemolytic streptococci and Clostridium spp [5]. We present the rare case of a patient presenting with carbapenem resistant Pseudomonas aeruginosa following a high pressure paint gun injury of the thumb. No study to date has demonstrated this type of infection in this patient population.

Initial injury; presentation of injection site 30 h after initial injury.
CASE DESCRIPTION
We present a case report of a 27-year-old male who sustained
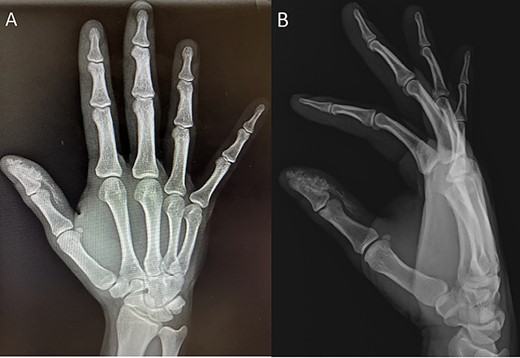
Initial injury radiographs; anterior–posterior (A) and lateral (B) radiographs of initial injury showing radiopaque material at the distal phalanx.
a high pressure injection injury with latex based paint to his right thumb secondary to a device malfunction. The patient was initially seen by providers at an outside facility and discharged on oral antibiotics. However, he presented at our facility 30 h after the initial injury with the inability to move his thumb due to significantly increased swelling and pain. Upon initial inspection, there was a 1-ml penetrating injury to the distal thumb (see Fig. 1). Initial X-rays demonstrated a radiopaque substance at the distal end of the right thumb coursing proximally without invasion of the tendon sheath (see Fig. 2A and B). The patient underwent emergent surgical incision, irrigation and debridement of the underlying tissues (see Fig. 3). Cultures were taken at the time of surgery and grew carbapenemase resistant Pseudomonas aeruginosa after 2 days. The patient was prescribed amoxicillin/clavulanate and ciprofloxacin for 7 days to provide appropriate coverage of the organisms isolated. The patient returned to clinic 1 week later where expressible paint material was found draining from the wound (see Fig. 4). The patient was admitted to the hospital and underwent a second I&D. Cultures taken at this time were negative for bacterial growth. The patient was discharged on amoxicillin/clavulanate and ciprofloxacin for 10 days. At 4 months, the wound was well healed with no signs of infection (see Fig. 5).

Initial irrigation and debridement; white paint can be seen invading the soft tissue, photo taken intraoperatively.

One-week post-op following initial I&D; white paint can be seen draining from surgical incision, photo taken at 1 week follow-up.

Follow-up; surgical wound seen healing well 14 weeks after second I&D.
DISCUSSION
We presented a unique case report where a patient presented 30 h after a high pressure injection injury. Cultures taken during initial incision, irrigation and debridement of the wound grew carbapenemase resistant Pseudomonas aeruginosa. Due to the limited number of reported cases of high pressure injection injuries and associated infections, we believe that more research is needed to determine the most appropriate management for these types of injuries.
The type of material injected plays a pivotal role in the severity of high pressure injection injuries and has been determined to be the single most important prognostic factor [1]. The injected material can cause a catastrophic inflammatory response resulting in tissue necrosis. Oil-based paint has been reported as one of the most toxic and severe with profound ischemia and rapid development of necrosis [3,6]. Additionally, animal studies have shown the induced inflammatory response secondary to the injected material ultimately results in an inhibition of the body’s ability to fight infection. This facilitates the growth of opportunistic bacteria such as Pseudomonas spp and Enterobacteriaceae found either natively or from injected materials.
Few studies discuss secondary infections associated with high pressure injection injuries. Literature supports the use of antibiotics however only one study has provided this recommendation based upon bacterial isolates from wound cultures. The study showed 47% of wound cultures were positive, with gram-negative bacteria found in 58% of isolates [7]. Microbial contamination was seen in 42% of patients in a review in 2006 by Hogan [3]. Most of these infections were polymicrobial and occurred even with the administration of antibiotics. Amputation rates in injuries with positive intraoperative cultures were identical to those with negative cultures [3]. A case report of a paint injection injury to the index finger reported cultures with gram-negative bacteria with the growth of Citrobacter freundii, Morganella morgani and Proteus vulgaris [8]. Other reports have demonstrated Enterobacteria following a high pressure paint injury; however, carbapenem resistance was not noted [7]. Carbapenem resistance has rapidly grown since its first reporting in literature in 1996 and has now become a major public health concern. Carbapenem antibiotics are often used as last resort and mortality from a carbapenem resistant bacteria strain is as high as 50% [9]. Infections by carbapenem resistant bacteria are predominantly obtained in the hospital setting; however, community acquired infections have increased in prevalence with percentages ranging from 5.6 to 10.8% in the USA. Various mechanisms of resistance have been observed including outer membrane porin changes altering intracellular drug concentration [10].
Steroid use following injection injuries have been shown to be beneficial in case reports; however treatment protocols vary, and no clinical trial has been conducted in this patient population. With the evidence of multidrug resistant organisms, such as carbapenem resistant Pseudomonas aeruginosa presented in our case report, steroids may be contraindicated in the treatment of high pressure injection injuries. Although steroids may help suppress the initial inflammatory response to injected materials, steroid use may significantly hinder the body’s ability to fight infection and administration should be cautioned [2].
In conclusion, high pressure injection injuries can lead to disastrous outcomes when not treated emergently with antibiotics, irrigation and debridement. With the emergence of multidrug resistant organisms, cultures should be obtained at initial debridement to provide optimal treatment against isolated organisms. Concerns should be raised as carbapenem resistant bacteria become more prevalent in the community, as evident by this case report.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}