





Abstract
Solitary fibrous tumor (SFT) is a rare mesenchymal neoplasm. It usually originates from the parietal pleura. SFT originating from the esophagus is exceedingly rare and even more so as a malignancy. We report a 57-year-old patient with a malignant 18 cm SFT of the esophagus that was treated with esophagectomy through a left thoracoabdominal incision. We discuss his surgical and oncologic management.
INTRODUCTION
Solitary fibrous tumor (SFT) typically originates from the parietal pleura. In the past, it was sometimes confused with mesothelioma; hence, the variety of names it has been called [1]. With the advent of immunohistochemical staining (IHC), it is recognized as a separate tumor [2]. SFTs are now known to occur throughout the body [3]. Despite the proximity to the pleura, SFT originating from the esophagus is very uncommon [4, 5]. It is a mesenchymal neoplasm, so in the esophagus, it originates from the submucosa. SFTs are typically benign but they can be malignant, which is defined as greater than four atypical mitoses per 10 high power fields (HPF) [6]. We report a particularly large and aggressive SFT of the esophagus, and performed surgical management and oncologic management once it recurred and spread.
CASE SUMMARY
A 57-year-old man developed dysphagia and progressive nonexertional chest pain leading to the discovery of a large malignant SFT of the distal esophagus occupying the majority of his left hemithorax. Upon evaluation at another academic center, the tumor was deemed unresectable and he received chemotherapy. He was referred to our center because of our experience with sarcoma and esophageal disease. He underwent five cycles of temozolomide with bevacizumab but had progression of disease. His treatment was switched to pazopanib. Unfortunately, after three cycles of pazopanib progression was again noted. At this point, he was referred to thoracic surgery for evaluation.
Imaging revealed tumor dimensions of 15–18 cm in diameter (Fig. 1). Following endoscopic ultrasound and positron emission tomography scan, a multidisciplinary board recommended surgical resection with esophagectomy through a thoracoabdominal incision. He was placed in a semirecumbent position. The costal margin was divided. The diaphragm was divided in a circumferential fashion leaving a rim of diaphragm on the chest wall. Gastric preparation was performed first (Fig. 2). Then, dissection was carried out along the mass into the chest. The mass was adherent to the pericardium and aorta but was encapsulated and not invading those structures. Multiple large aortoesophageal vessels were divided with the Ligasure vessel sealer device (Medtronic MN, etc.). The left lower lobe and inferior pulmonary vein were splayed across the mass. Inadvertent injury of a branch of the inferior pulmonary vein required vascular repair. The mass emanated from the lower one-third of the esophagus (Fig. 3). The esophagus was divided at the level of the left inferior pulmonary vein and the mass removed. Frozen sections of the esophagus, surrounding pleural, pericardium and lung, were performed and were negative. The anastomosis was performed in a typical fashion with a circular end-to-end stapler. The diaphragm was reapproximated, and the extra conduit length was tacked down into the abdomen. The immediate postoperative course was largely uneventful, with negative radiographic leak test performed on postoperative Day 5 and the patient discharged to home on postoperative Day 7.
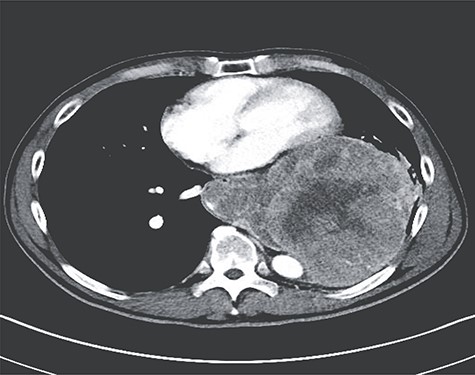
Axial image from preoperative CT of the chest demonstrating extension from esophagus and relation to the pericardium and thoracic aorta.
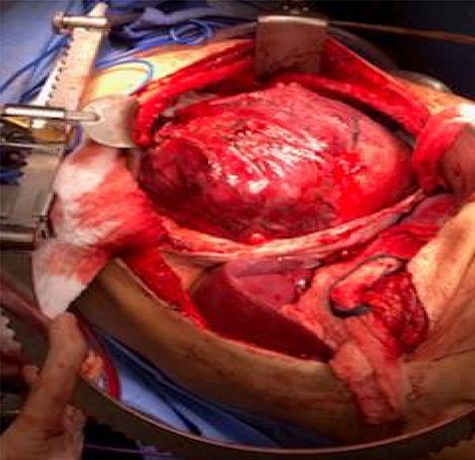
Thoracoabdominal exposure of esophageal SFT.
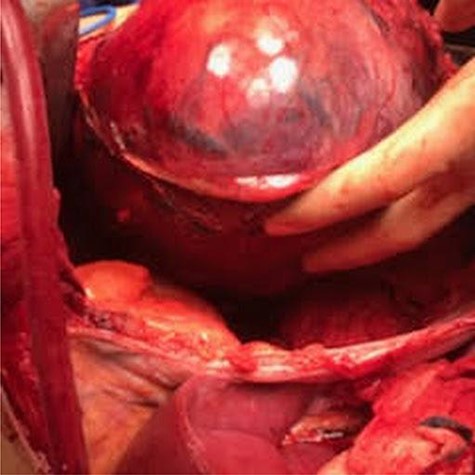
Dissecting the tumor from the chest cavity.
Pathologic evaluation demonstrated an 18 cm, 2 kg tumor emanating from the submucosa of the esophagus (Fig. 4). Remarkably, the mucosa remained intact. Periesophageal, gastric, hilar and mediastinal lymph nodes were negative. Margins were confirmed negative. There were 42 mitoses per HPF with 30% necrosis and histologic grade 3. Tumor markers showed positive for CD34, vimentin, BCL-2 and beta-catenin (membranous pattern); weakly positive for caldesmon and negative for CD31, DOG1, CD117, S100, smooth muscle actin, desmin and pancytokeratin. Foundation One testing revealed microsatellite status stable and tumor mutational burden low. Genomic findings revealed STAT6-NAB2-STAT6 fusion and TP53-Y205C (Fig. 5).

Eighteen-centimeter size tumor, 2 kg in weight.
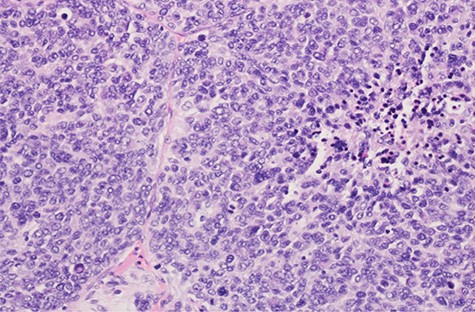
Microscopic pathology of the tumor.
Surveillance scans were negative until 9 months later when multiple bilateral pulmonary nodules were discovered (Fig. 6). Biopsy of one of the nodules revealed recurrent, metastatic disease. He was treated with pembrolizumab for three cycles but had progression. He was then switched to gemcitabine and docetaxel for three cycles but had progression. Most recently, he underwent six cycles of doxorubicin, which showed stable disease.

One-year postoperative CT showing metastases to the lungs.
DISCUSSION
SFT of the esophagus was first described in 1931 [7]. Most patients with esophageal SFTs present with dysphagia. Leiomyomas and GIST tumors may look similar on barium swallow and endoscopic ultrasound. Biopsy is easily obtained with endoscopy. SFTs histology characteristics are patternless bundles of spindle cells and collagen. IHC markers are CD34 positive and CD 117 negative, which differentiates them from GISTs tumors [8]. Malignancy is reported in only 10–15% of thoracic SFTs and is associated with tumors >7 cm [9]. Surgical resection is the treatment of choice when feasible. We did not give adjuvant radiation therapy given what appeared to be a clean resection with negative margins. We also did not give adjuvant chemotherapy given the paucity of data with this tumor and unclear benefit. Clinicopathologic parameters are currently used in risk prediction models for SFT, but the molecular determinants of malignancy in SFTs remain unknown, Bahrami et al. showed that TERT promoter mutations were strongly associated with high-risk clinicopathologic characteristics and outcome. An adverse event (relapse and death) occurred in 16 of 68 (24%) patients of their targeted study [10]. Like management of other sarcomas, a multidisciplinary approach to malignant SFTs is warranted. With such a large, malignant tumor, such as this, we would probably give adjuvant chemotherapy next time. The thoracoabdominal approach was an excellent choice for this patient as the tumor was difficult to extract even through this large incision. Surgical resection improved his quality of life by giving him back the ability to swallow and undoubtedly improved his survival.
CONFLICT OF INTEREST STATEMENT
None.
DISCLOSURES
The authors have nothing to disclose.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}