





Abstract
Herniation pits are small benign oval lesions that were reported to be always lying within the super-lateral femoral neck, and were first described in 1982 by Michael J. Pitt. They are usually a unilateral incidental finding along with asymptomatic course. It was widely believed that herniation pits are a result of invagination of the overlying synovium into small cortical defects in the femoral neck. In our case; the mentioned lesions were found atypically bilaterally at the inferomedial aspect of the neck of femur of a 7-year old child. Radiological scans were efficient to obtain an adequate diagnosis whereas conservative management proved to be sufficient dealing with the lesions. Synovial pits may have atypical clinical and radiological course, and this can raise concerns especially with symptomatic hip that may encourage surgical interventions. However, due to benign course of these lesions, we do not recommend any surgical intervention for such lesions.
Introduction
Radiolucent round lesions which are usually less than 1 cm diameter surrounded by a thin rim of sclerosis is often identified in the proximal superior part of femoral neck. Although usually recognized as incidental and benign, this radiolucency may be of clinical concern in patients with hip symptoms.
Incidence of the synovial pits was reported around 5% of the general population. In the early 80’s Allen H. described bony depression in the supero lateral quadrant of the femoral neck as “the cervical fossa of Allen” [1]. Young adults and children can demonstrate a small depression in this region; however, the majority of adults will demonstrate a plaque-like bony elevation surrounding and invading into the fossa of Allen [2]. Initially, this area was named the “reaction area” by Angel in 1964 [3]. Subsequently, Pitt described a cavity, which developed underneath the reaction area via herniation of synovium and soft tissues through perforations or defects in the reaction area, through mechanical forces of the overlying joint capsule [4]. Latest evidence from leaning suggested that femoro-acetabular impingement may have a role in their aetiology [5,6].
In our case reported, as it came to our knowledge is the first in the literature to investigate into these radiological findings in a skeletally immature patient. In addition, the atypical infero medial site of the femoral neck would contribute to further investigation for the main aetiological factors that can develop these herniation pits especially in paediatric and children age group.
Case Report
A 7-year-old boy presented to the emergency department of our hospital complaining of left hip joint pain and inability to bear weight after a trivial fall one day earlier. He had history of mild left hip pain of 3 weeks’ duration which aggravated after his trivial fall sustained by push from a colleague. There was no history of fever, altered sensorium or any other joint pain. No family history of similar illness.
Examination revealed decreased flexion 0–80 degree, internal rotation 0–20 degree and external rotation 0–35 degree, unable to do straight leg raise due to pain, with no swelling or erythema, no tenderness with positive Patrick (impingement) test with intact neurovascular status.
Patient was given adequate analgesia and routine blood tests were done (CRP 5.8 WBC 7.5x109). X-rays revealed small Lytic lesion with surrounding sclerosis at infero-medial aspect of left femoral neck in antero-posterior and lateral views (Fig. 1, 2).

Showed AP view of the pelvis.

Showed lateral view of the hips with pelvis.
CT hips reported a well-defined lesion seen bilaterally in the neck of femur anterior infero-medial aspect, more prominent on the left side measuring 7 x 3 mm on left side both in coronal (Fig. 3) and axial (Fig. 4) views. On the right side, other lesion measuring 2 x 1 mm (Fig. 5) seen in coronal view. These two lesions are well defined with a sclerotic border with a small cortical defect. The lesion shows fat density. The symmetrical appearance of the lesion combined with the fat density and location suggest the diagnosis of synovial herniation pit. MRI Pelvis revealed minimal left hip joint effusion with loculated fluid seen along the trochanteric bursa with the largest measuring 0.9 x 1.5 cm (Fig. 6, 7).
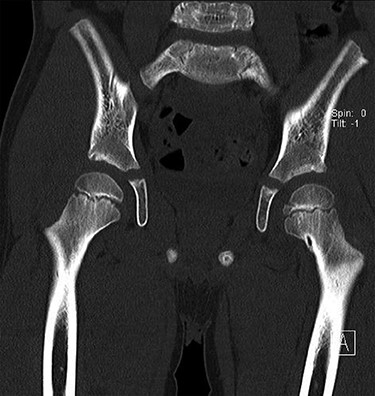
Sowed coronal cut of CT hips demonstrating the synovial pit on left and right side.
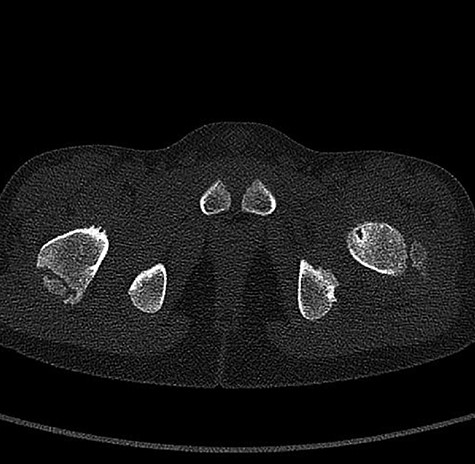
Showed axial cut of CT hips demonstrating the synovial pit on left and right side.
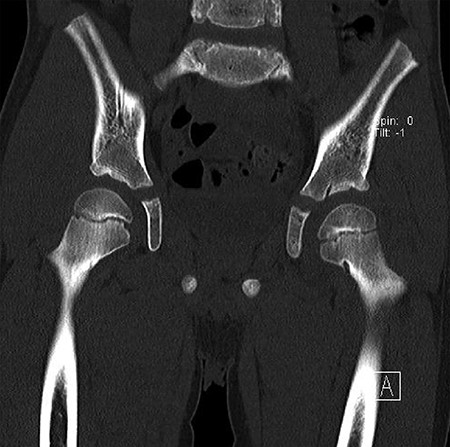
Showed coronal cut of CT hips demonstrating the synovial pit prominent right side.

Showed T2 signal MRI coronal cut.
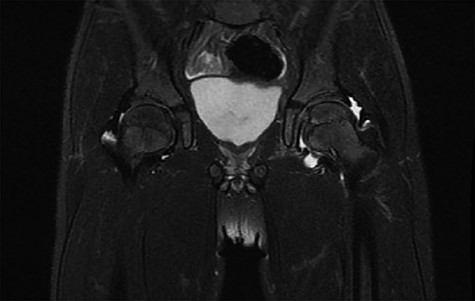
Showed T1 signal of MRI hips.
Follow-up of the case showed complete regression of the symptoms. Patient was full weight-bearing and performing daily activities with no pain, straight leg raises up to 90 degrees, Range of motion was fully painless with flexion 120 degrees, while extension, abduction and external rotation were 20, 40 and 35 degrees respectively (Figure 8, 9).

Showed full active flexion of the left hip joint.

Showed external rotation of the left hip joint.
Follow-up X-ray showed regression of the lesion in the form of progression of the dense sclerosis of the defect of the left femur while the right femur neck lesion is barely visible (Figure 10) and advised for watchful waiting.

Follow-up AP x-ray pelvis and hips.
Discussion
Herniation pits of the femoral neck are benign bony lesions or defects which are located in the predominantly located in the supero lateral aspect of the femoral neck. While there are no reported incidence rates in the paediatric population, it is said to be around 5% in the adults of an average rate. Where patients were predominately male and the average age was 45 years [7]. Most herniation pits are found incidental findings and not associated with obvious clinical symptoms [8].
Aetiology to these lesions were contributed initially to focal cortical defects through the so called “reaction zone” in the zona orbicularis. That said to be filled through Herniation of these fibrous and/or cartilaginous tissue and fluid elements into spongy bone under the pressure and mechanical abrasion of the anterior hip capsule, adjacent ilio-femoral ligament and overlying iliopsoas muscle [8]. As most of the reported cases in literature were highly active skeletally mature patients as joggers or dancers. It is possible that the appearance of these pits is correlated with physical activities and hip joint movements that might be a major contributing factor [9].
The differential diagnosis of those lesions may include but not limited to osteoid osteoma, intra osseous ganglion, focal avascular necrosis, and atypical metastatic lesions [10]. CT is always the cornerstone scan for detecting these subcortical lytic synovial pits which are usually surrounded by sclerotic margins [10,11]. Thus adequate diagnosis through computed tomography (CT) and magnetic resonance imaging (MRI) of the hips would avoid unnecessary surgical intervention or biopsy.
Despite some papers that had promoted for intervention for symptomatic pits including intra articular corticosteroid injection [11], arthroscopic debridement and surgical curettage of the pits [12]. There is a limited evidence in the literature that supports any surgical intervention including curettage or biopsy to confirm the diagnosis of the pits or to manage symptomatic pits especially in paediatric population. Furthermore, our patient’s clinical and radiological symptoms faded away with conservative treatment.
In conclusion, Herniation pits are troublesome to physicians in practice. There are no adequate studies to understand either the nature or the aetiology of the lesions. Atypical age groups are prone to development of these lesions. However, it is not sufficiently reported in the literature. CT scans are mandatory to confirm suspicious lesions and to exclude other troublesome differential diagnosis. Adequate diagnosis may save unnecessary surgical interventions. Conservative management and watchful waiting are the mainstay of treatment.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}