





Abstract
Thymolipoma is a rare benign slow-growing encapsulated tumor of anterior mediastinum that accounts for 2–9% of all thymic neoplasms. About 30–50% of them are asymptomatic and found incidentally. Less than 200 cases have been published in the world literature so far. Here we report a case of thymolipoma of an adult female presented with progressive dyspnea, chest tightness and non-productive chough for 2-month duration. All blood investigations were normal. Radiological examinations suggested the presence of fat and soft tissue within the tumor without invading the neighboring structures. We concluded that the only curative treatment of thymolipoma is surgical excision. Unfortunately, the patient did not give consent despite telling her the outcomes if we do not do the surgical procedure, and a week later she passed away due to respiratory distress secondary to the mass effect of the tumor.
INTRODUCTION
Thymolipomas are very rare benign tumors of the thymus first reported by Lange in 1916 and further coined by Hall in 1949 that consist of mature adipose cells and thymus tissue. Thymolipoma accounts for 2–9% of all thymic neoplasm. Less than 200 cases have been published in the world literature, and its incidence in both genders is equal and usually develops at any age [1]. This tumor can be associated with chronic lymphocytic leukemia, myasthenia graves, aplastic anemia, hyperthyroidism and Hodgkin’s disease. The majority of these patients were diagnosed incidentally and complete surgical excision is curative treatment [2].
CASE REPORT
A 60-year-old female patient presented to the emergency with complains of dyspnea, non-productive cough and chest pain for 2 months. There is no history of hemoptysis, weight loss and substance abuse. On physical examination, oxygen saturation was 64%, blood pressure was 170/110 mm Hg, temperature was 97.9°F (36.6°C) and blood sugar was normal. Local examination of the chest revealed limitation in chest movement and decreased tactile focal fremitus on both sides of the chest. On percussion, dullness on both sides of the chest was noticed. On auscultation, decreased breath sounds on both sides of the chest were detected and the apex beat of the heart was displaced on the right side. The blood tests performed in the emergency room were in normal range. She underwent radiological evaluation with chest X-ray that revealed diffuse infiltration on both lungs (Fig. 1). Thoracic echocardiography revealed huge mediastinal mass with dextrocardia. This was followed by chest computed tomography (CT) that showed bilateral diffuse mediastinal mass, which involves fatty tissue containing soft tissue streaks that probably represent islands of normal thymic components with no infiltrations (Figs. 2–3). We concluded that the only curative treatment of thymolipoma is surgical excision. Unfortunately, despite the patient being told about the surgical procedure, she did not give the permission and passed away a week later due to secondary compression to the lungs.
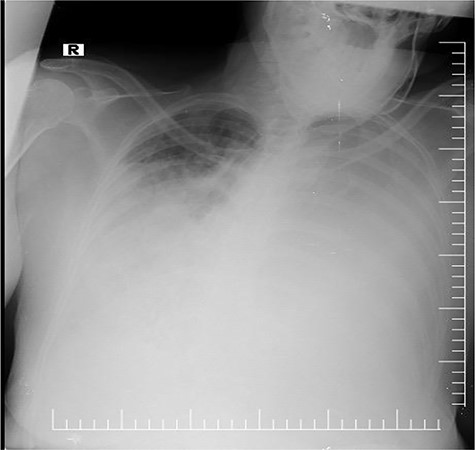
Chest X-ray revealing bilateral opacity in the mediastinum mimicking pulmonary edema.
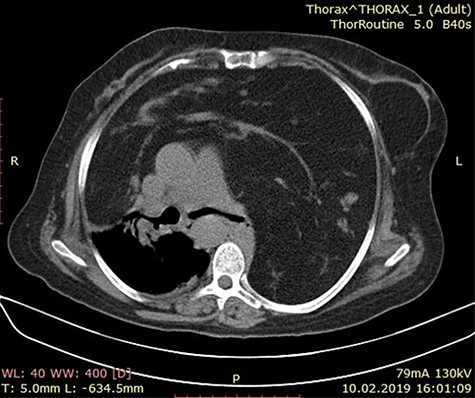
Axial chest CT image showing a mass lesion with wide range of fat density filling both hemithorax was observed, including linear and nodular densities in the right hemithorax. A dense retrosternal mass displacing both lungs and chest. No evidence of invasion is seen.

CT scan of the chest showing a large anterior mediastinum mass projecting to the right and left hemithorax with wide range of fat tissue density.
DISCUSSION
Thymolipoma is a very rare benign tumor of the thymus and first reported by Lange in 1916 and further coined by Hall in 1949 that consists of mature adipose cells and thymus tissue. Thymolipoma accounts about 2–9% of all thymic neoplasm. Less than 200 cases have been published in the world literature, and its incidence in both genders is equal and usually develops at any age [1]. In some cases, thymolipoma can be associated with chronic lymphocytic leukemia, myasthenia graves, aplastic anemia, hyperthyroidism and Hodgkin’s disease [2]. In our case, there was no association between this presenting case and the above-mentioned tumors. In thymolipoma, half of the patients are asymptomatic, and incidentally the mass is discovered radiologically. The other half mostly represents shortness of breath, cough, chest pain and upper respiratory tract infection [3]. Our case has similar features to those reported above. The etiology of thymolipoma remains unclear. In the past, some theories have explained this, such as hyperplasia theory that suggests diffuse thymus hyperplasia, which is replaced by fatty tissue, and mixed tumor theory that explains the mixed tumor of endoderm and mesenchymal origin [4, 5]. The diagnosis of thymolipoma should be considered in the accuracy of an anterior mediastinal mass with fatty tissue containing soft tissue streaks that probably represent islands of normal thymic components on CT scans [5]. The CT scan in this case report showed a similar finding of a bilateral diffuse mediastinal mass, which involves fatty tissue containing soft tissue streaks that probably represent islands of normal thymic components. Although biopsy was technically feasible, it is not indicated in these cases because the mass must be surgically removed. The only curative treatment of thymolipoma is surgical excision with no recurrence and malignant transformation with a good prognosis. In our knowledge, this is the first reported case in Somalia.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}