





Abstract
We present a case of incorrect seating of the polyethylene liner in an INFINITY total ankle replacement causing discomfort and eventually leading to a revision ankle replacement. This malposition of the implant was observed on a computed tomography (CT) scan as a ‘gap’ between the liner and the body of the replacement. The patient complained of discomfort on walking postoperatively, which limited activity. All investigations were normal including X-Ray, inflammatory markers, ultrasound, and it was only the subtle CT changes along with history that confirmed the diagnosis. This case demonstrates a complication of the design of the INFINITY prosthesis and the approach taken to the ankle when inserting. The patient fortunately made a full recovery after revision surgery, returning to normal activities with minimal pain.
INTRODUCTION
Although total ankle replacement (TAR) is an increasingly common procedure in specialist foot and ankle units, the number of ankle replacements remains fewer than hip and knee. Current TARs are either two- or three-component designs. INFINITY, which is a fixed bearing implant, has rapidly become the most common prosthesis since its introduction in 2014 and had a market share of 51% in 2018 [4]. Dislocation of the insert is a known complication in mobile bearing implants. Complications associated with the locking mechanism are incorrect seating, disengagement, failure of the locking mechanism and dislocation or subluxation of the poly component. We report a case of inadequate seating of the poly component in an ankle replacement leading to persistent pain and subsequent revision.
CASE REPORT
A 56-year-old man underwent TAR due to post-traumatic osteoarthritis using an ‘INFINITY’ TAR (Wright medical implant, size 4 tibial tray, size 3 talar component and 9 mm poly component).
His initial postoperative period was uneventful. Postoperative X-rays showed good alignment and implant position. Over the following months, he complained of persistent medial and posterior ankle pain. On examination, he had minimal swelling over the medial side of the ankle. His range of movement was 20 degrees of dorsi-flexion and 30 degrees of plantar-flexion, which was painless. He had no rest pain but described something ‘pressing inside’ limiting his walking distance.

CT demonstration of the poly liner sitting slightly outside of its groove ‘the gap sign’ (A) Lateral view showing ct gap sign (B). AP view showing gap (C). AP view showing poly seating.
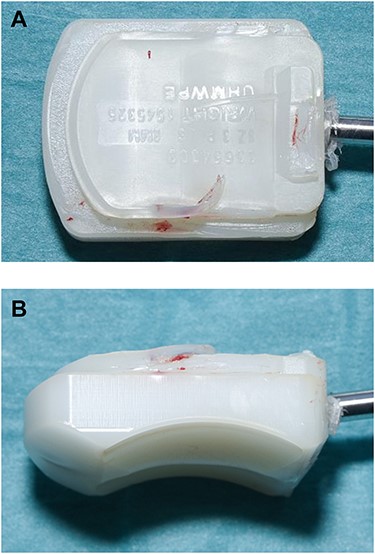
(A, B) Intraoperative pictures of polyethylene liner demonstrating incomplete seating into replacement.
All inflammatory markers were within normal limits. Upon suspicion that the talar component might be irritating the tibialis posterior tendon, he underwent an ultrasound which was normal. His computed tomography (CT) was reported as normal by the radiologist. Symptoms suggested possible impingement of a slightly oversized talar component on medial malleolus. On close scrutiny, it was apparent that the CT postoperatively showed the poly to be seated anteriorly with a failure to engage posteriorly, leaving a void in the socket. We describe this as a ‘CT GAP sign’ (Fig. 1A–C), and he was offered a revision ankle replacement.
Revision ankle surgery was undertaken by anterior approach through the previous incision. Intraoperative samples were taken which ruled out infection. The tibial component was well fixed to bone and showed no evidence of loosening, subsidence or rotational malalignment. Macroscopic examination of the retrieved insert showed grooves on its side. The poly was not fully reduced in its groove and had dislodged from the groove subsequently on the posterior aspect of the implant (Fig. 2A and B). He had a revision of the talar component to size 2 and change of polythene with good clearance of his medial gutter.
DISCUSSION
Cases of polyethylene component dislocation due to trauma in total knee replacements have been reported; Voskuij et al. described a case series of nine patients showing insert dissociation after fixed bearing, posterior stabilized, constrained Genesis total knee replacements [1]. Real incidence of inadequate seating of poly component in an ankle replacement is unknown. To the best of our knowledge, this is the first case of an INFINITY ankle replacement requiring revision due to persistent pain and stiffness following a failure to seat the polyethylene component.
Noelle et al. evaluated 100 ankle replacements using third generation, STAR® ankle prosthesis, which include a minimally constrained design utilizing a mobile meniscal-bearing polyethylene insert, uncemented fixation and a three-component design [2]. The authors describe a case of ankle replacement complicated by dislocation of poly component needing revision. Hinterman et al. reviewed a series of 117 ankle replacements in which a total ankle arthroplasty failed after a mean of 4.3 years and was revised with a HINTEGRA three-component total ankle prosthesis [3]. HINTEGRA is also a mobile bearing poly component design. He found one case of complication due to dislocation of poly component. Hoffman and Fink after a systematic search of literature since 2000 evaluated 26 papers with a total of 1318 follow-up ankle prosthesis [5]. Of 1318, a total of 188 were surgically revised, out of which seven were due to dislocation of inlay i.e. 0.53%.
Dislocation or inadequate seating of poly component in an ankle arthroplasty is a rare complication. Of 4687 TARs reported in NJR in 2017, there were four cases of meniscal insert dislocation leading to revision [4].

Inserter assembly.
The cause of inadequate seating may be due to technical error, failure of the poly inserting mechanism or failure of design of the locking mechanism in the INFINITY implant. It may also be possible to postoperatively dislodge the poly component. The poly inserter does not give a visual confirmation of seating as it is not possible, in the INFINITY replacement, to visualize the back of the component using the standard anterior approach. Incorrect seating of poly may lead to eccentric overloading of joint space, eccentric poly wear and mechanical pain.
The polyethylene inserter assembly consists of the poly inserter, a guide rail and attachment screw (Fig. 3). The guide rail inserts onto the poly inserter, and the handle is pulled back and locked into a start position. Whilst inserting, the dovetail feature of the implant slides into the guide rail ensuring correct antero posterior orientation of component. Then, the assembly slides over attachment screws and flush to the surface of the tibial tray after securing the attachment nut. Incorrect technique, unmatched tibial and talar cuts or inadequate ligament balancing can lead to incorrect seating. There is, unfortunately, no radiological marker to confirm poly position in this implant.
We would advise adequate exposure, clearing of soft tissue and thorough lavage along with attention to detail whilst preparing the poly insertion assembly. Addition of a radiological marker as in the knee would help early recognition. Infinity is the most commonly used implant in TARs in the UK and gaining more popularity; surgeons should keep in mind this rare complication, and early CT should be considered in cases with persistent pain postoperatively. In conclusion, incorrect seating of poly component is a rare complication, which can be a cause of persistent pain in ankle replacements. This can be easily missed by the untrained eye even on CT scans. Prompt revision is needed to prevent late consequences.
Conflicts of Interest statement
The authors declare no conflicts of interest.

{kind=link}
{kind=link}
{kind=link}