





ABSTRACT
Jejunoileal diverticula (JD) are an uncommon condition most prevalent in the sixth and seventh decade of life. Although mostly asymptomatic, JD can be complicated by perforation, diverticulitis, abscess, bleeding, fistula, and small bowel obstruction (SBO) secondary to enterolith formation. There are a limited number of cases describing JD complicated by SBO secondary to enterolith formation. Most of these cases are not associated with diverticulitis and multiple JD are present in all but one previously reported case. We present a case of diverticulitis of a large, isolated jejunal diverticulum complicated by de novo enterolith-induced SBO initially diagnosed as intussusception based on computerized tomography (CT) imaging. Our main objective is to increase awareness that isolated JD are not as readily evident on imaging as cases presenting with multiple JD, but nevertheless should be considered as possible etiology of acute abdomen.
INTRODUCTION
Jejunoileal diverticula (JD) are a rare condition characterized by herniation of mucosa and submucosa through the muscular layer of the bowel wall [1]. JD are present in approximately 1–5% of the general population but are most prevalent in patients between 60–70 years old [2, 3]. Etiology of JD seems to be multifactorial as evidenced by the multiple pathological processes associated with the development of JD, including systemic sclerosis, visceral myopathy, and visceral neuropathy of intestinal wall [4]. Eighty percent of JD are in the jejunum; these tend to be large, multiple, and are located on the mesenteric side because diverticula form at sites where blood vessels penetrate the intestine [5, 6]. Most patients with JD are asymptomatic; however, chronic symptoms associated with JD are abdominal discomfort, fullness, abdominal cramping, and anemia due to iron or vitamin B12 deficiency secondary to malabsorption. Complications occur in up to 10% of patients with JD; these include perforation, diverticulitis, abscess, bleeding, fistula, and small bowel obstruction [2, 5]. We present a case of diverticulitis of a single, large jejunal diverticulum complicated by small bowel obstruction caused by a de novo enterolith.
CASE
An 86-year-old male previously treated for hypertension presented to the emergency department with two days of sudden abdominal pain and nausea which resolved temporarily after self-induced emesis. Patient was examined and investigated thoroughly. Temperature was 36.3 C, blood pressure was 138/81, and pulse was 78. Physical examination revealed a tender, firm and distended abdomen with hyperactive sounds. Laboratory analysis revealed hemoglobin at 10.3 g/dL, leukocytes 3.1 K/cmm, urea nitrogen 19 mg/dl, creatinine 0.6 mg/dl, sodium 137 mmol/l, potassium 3.6 mmol/l, chloride 104 mmol/l, bicarbonate 24 mmol/l, calcium 8.6 mg/dl, total protein 6.3 g/dl, albumin 3.1 g/dl, total bilirubin 0.7 mg/dl, alkaline phosphatase 98 U/l, SGOT 20 U/l, SGPT 27 U/l. Laboratory values were consistent with patient’s previous clinic visits. Computed tomography (CT) of the abdomen revealed a fluid-filled, significantly dilated stomach as well as multiple dilated loops of small bowel with air-fluid levels consistent with mechanical small bowel obstruction caused by intussusception of small bowel (Fig. 1). After initial fluid resuscitation and antibiotic administration, consent was obtained for emergent exploratory laparotomy. The exploratory laparotomy revealed a 3.0 × 2.5 cm intraluminal calculus in the ileum responsible for the small bowel obstruction, without evidence of intussusception (Fig. 2). The obstructing enterolith was ‘milked’ proximally until it reached, and subsequently ‘fell into,’ an isolated 6.0 × 3.0 cm jejunal diverticulum which had not been previously noted on CT imaging. The enterolith was removed along with the segment of the jejunum containing the isolated diverticulum, which was the source of the enterolith (Fig. 3). On histologic examination, the mucosa of the extracted diverticulum was found to be granular and erythematous; the remaining small bowel had marked mucosal ulceration and near-transmural inflammation with granulation tissue. Hospital course was complicated by decreased urine output that resolved after fluid resuscitation. On the fourth postoperative day, nasogastric tube was discontinued, diet was advanced and tolerated, and the patient was discharged. Review of the patient’s CT scan of the abdomen revealed the isolated jejunal diverticulum that was consistent with the excised diverticulum (Fig. 4).
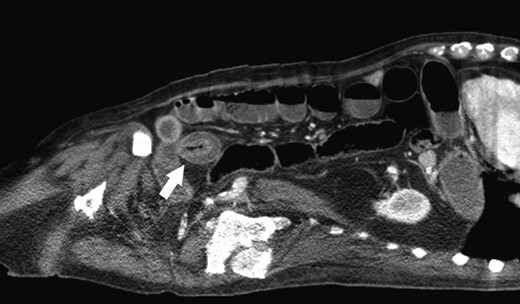
Enterolith-induced small bowel obstruction resembling intussusception (white arrow).
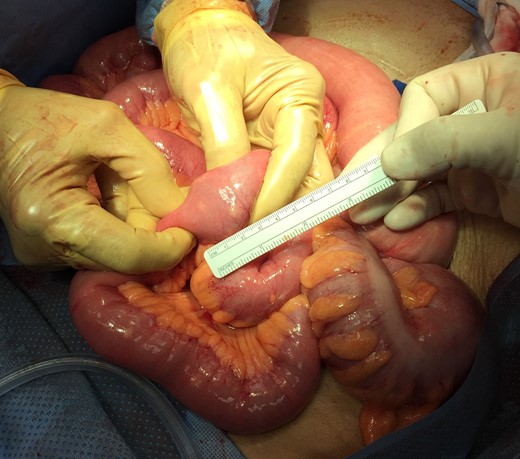
Jejunoileal small bowel obstruction secondary to enterolith without evidence of intussusception.

Resected specimen of jejunum with isolated large diverticulum and enterolith.
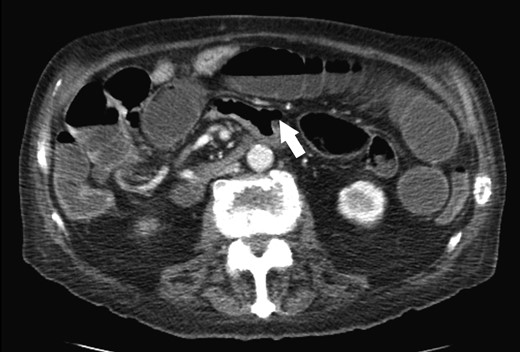
Isolated diverticulum in jejunum (white arrow).
DISCUSSION
Jejunal diverticulosis complicated by enterolith formation is rare. Enteroliths are classified as primary or secondary. Primary stones are formed within the intestine, while secondary stones are introduced from outside the gastrointestinal tract such as the gallbladder or kidney [7]. True primary stones can be formed de novo from bile precipitation that occurs due to pH changes and dyskinesia that occurs within the diverticula; false primary stones can form as a result of undigested food entrapped within the diverticula [7, 8]. Once stones are formed, they can dislodge from diverticula into the intestine and cause obstruction. Most cases of small bowel obstruction due to enterolith are not associated with concurrent diverticulitis. Small bowel obstruction due to enterolith associated with jejunal diverticulitis have been previously described, however the patients presented in these reports had diffuse jejunoileal diverticulosis, or presented with multiple jejunal diverticula [8, 9]. The case presented occurred in a patient from the Navajo Nation of Northeastern Arizona. To our knowledge, only one case of small bowel obstruction by enterolith associated with diverticulitis of a single jejunal diverticulum has been previously documented in Europe [10]. We present this case as the first to be documented in the United States and hope it serves as additional evidence that a single jejunal diverticulum, not just diffuse jejunoileal diverticulosis, may lead to enterolith formation and subsequent small bowel obstruction, and therefore, should be included in the differential of cases of acute abdomen. We also present this case due to the peculiarity of being readily misdiagnosed as intussusception with a prominent ‘target’ sign and the ease by which isolated jejunal diverticula may be missed on initial reading of imaging. Cases of intussusception secondary to enterolith formation in JD have been described in literature, so an additional consideration of this case could be that intussusception may have been present at time of imaging that could have resolved by the time of exploratory laparotomy, however, we did not find edema or signs of compromise in the intestine adjacent to the obstruction that would indicate that the enterolith acted as a lead-point for intussusception. Additionally, we recommend that gallbladder, kidneys, and ureters are inspected, as these could be rare sources of small bowel obstruction that have been previously documented in literature as well.
ACKNOWLEDGMENTS
The authors gratefully thank the editorial contributions of Gabino G. Trejo, Nicole E. Bejany, and Cazandra Zaragoza.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES

{kind=link}
{kind=link}
{kind=link}
{kind=link}