





Abstract
A 6-year-old male was seen for evaluation of middle ear polyp with associated hearing loss and otorrhea. CT scan revealed canal polyp with a stalk extending to the middle ear with malformation of the malleus and incus. The patient underwent exploratory tympanotomy which revealed a fistula from the bony-cartilaginous junction connecting to a middle ear mass which had eroded the incus. Intraoperative pathology suggested columnar epithelium without cholesteatoma or muscle. Final pathologic diagnosis reported dense fibrous tissue as well as ectopic salivary gland tissue, consistent with salivary gland choristoma. After removal of the mass, a partial prosthesis was successfully placed. Middle ear salivary gland choristoma is a rare entity. It can be confused clinically with cholesteatoma and is usually diagnosed on pathology. This diagnosis is often associated with other external, middle, and inner ear abnormalities.
INTRODUCTION
Heterotopia is the phenomenon of normal tissue in an abnormal anatomic site. These tissues are most often benign. Choristoma, a type of heterotopia, is a rest of histologically normal tissue in an embryologically abnormal site. Choristomas are rare in the middle ear and were first described by Martin in 1961 [1]. Most of the reported cases, involving the middle ear, present in children and adolescents, with a slight female predominance [2]. These tumors have also been reported in other areas of the head and neck [3]. Buckmiller et al. conducted a thorough review of the cases reported up until 2001 [4]. Since that time there have been fewer than 10 published reports of salivary gland choristoma. The described cases present with unilateral conductive hearing loss due to mass effect, in addition to variable tinnitus and otorrhea. The lesions are more common on the left side. Many cases also present with a visible mass in the middle ear. Due to the infrequency of middle ear choristoma, the diagnosis is unsuspected until surgical pathology is obtained. The majority of cases are associated with facial nerve dehiscence [4], much more frequently than in seen cholesteatoma cases. These lesions may be associated with syndromic developmental abnormalities. Branchial arch abnormalities are commonly associated with choristoma, including deformities in stapes suprastructure and malformation of long process of incus [5]. The salivary tissue found in these lesions has both serous and mucinous components. Here we describe a case of choristoma along with associated surgical, clinical, histological, and radiographic findings.
CASE PRESENTATION
A 6-year-old male was referred to our clinic by an outside physician for evaluation of a ‘middle ear polyp’. He was initially referred to the outside physician for a growth in the left ear canal with associated decreased hearing and otorrhea. Audiogram at the outside office revealed left mixed hearing loss and right sensorineural hearing loss (Fig. 1). Past medical and surgical history was significant for removal of a ‘skin tag’ from the left ear shortly after birth and expressive speech delay. The child was otherwise healthy with an unremarkable birth history.
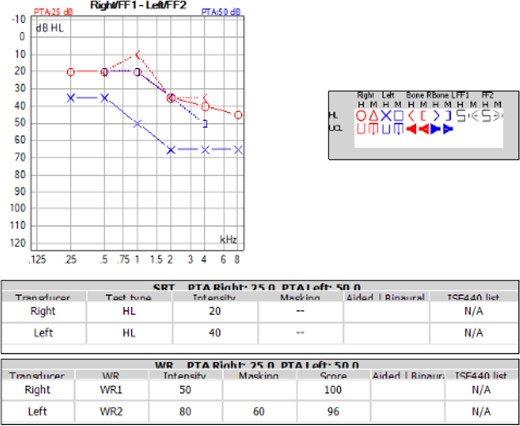
Audiogram of the patient showed left sided mixed hearing loss and right sided sensorineural hearing loss. Word recognition was normal bilaterally.
The outside physician removed the ear canal polyp in the operating room, noting it arose from the superior bony-cartilaginous junction. At the time of surgery, a possible posterior-superior middle ear mass was visualized. The patient was then referred to our office. The patient complained of one year of left hearing loss, left tinnitus, and intermittent left vertigo. Examination revealed purulence emanating from the superior aspect of the bony-cartilaginous junction. No middle ear abnormalities were visible.
Computed tomography (Fig. 2) revealed the ear canal polyp with a stalk extending to the middle ear. A fistula was seen in the external auditory canal. Also seen were ipsilateral malformed malleus and incus, a small epitympanum, and either thickening of the tensor tympani tendon into the mass or lack of tensor tendon.

CT of the temporal bones without contrast, with bone windowing. (A) Axial scan showing the mass extending into the middle ear, past the ossicles and toward the eustachian tube. (B) Coronal scan revealing the fistula of the external auditory canal (arrow), with the mass extending from that area into the middle ear. (C) Coronal scan with small epitympanum and ossicular view.
The patient underwent exploratory tympanotomy which revealed a fistula from the superior bony-cartilaginous junction connecting to a middle ear mass. The mass traveled under the long process of the incus toward the eustachian tube. The ossicles were malformed, including a very tight epitympanum containing the heads of the malleus and incus. The incus was seen to be almost completely eroded by the mass and was therefore partially removed to facilitate removal of the mass. However, the head of the incus could not be removed due to the tight attic. The mass itself had the gross appearance of muscle, and at one point it was considered to be an abnormality of the tensor tympani. However, intraoperative pathologic examination of the tissue was suggestive of columnar epithelium without cholesteatoma or muscle. After partial removal of the mass down to near the Eustachian tube orifice, a partial prosthesis was successfully placed. The patient did well postoperatively.
Final pathologic examination (Fig. 3) showed dense fibrous tissue with focal benign glands as well as ectopic salivary gland tissue with overlying excoriation.
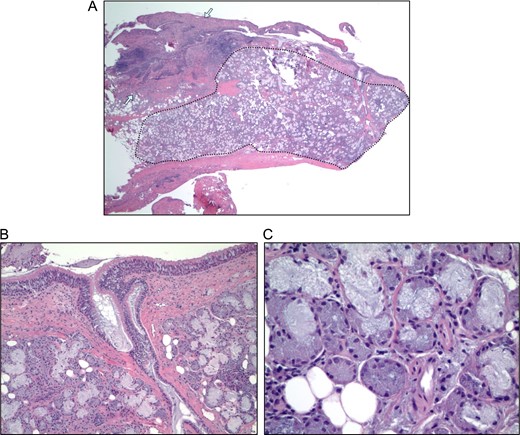
Hematoxylin and eosin (H&E) stained micrographs of the specimen. (A) Low power H&E of the specimen, showing areas of fibrosis (between arrows) and glandular tissue composed of serous and mucinous cells typical of submandibular salivary gland (surrounded by dotted line). (B) Higher power H&E shows the salivary glandular tissue with connection to the surface (bottom portion of image) and overlying ciliated columnar epithelium (at top of image). (C) High power H&E shows the admixture of cell types with the darker granular serous cells and the pale blue mucinous cells.
DISCUSSION
Benign salivary tissue in the middle ear is a rare diagnosis with less than 50 reported cases in the literature. Choristoma is a term used to describe a benign collection of tissue formed by its germ cells in an ectopic site. This is to be differentiated from hamartoma which describes a collection of tissue normally found at that site growing in an abnormal fashion. In this case, the presence of salivary tissue in the middle ear is thought to arise from an abnormality in development. The exact nature of this abnormality is currently unknown. Many of the case reports note a location near the horizontal portion of the facial nerve, often with associated dehiscence of the Fallopian canal. Embryologically, the first and second branchial arches are responsible for creating the mandible and much of the ossicular chain. It is known that ectopic salivary tissue can involve the posterior mandible as a so-called ‘Stafne’ cyst, and there are case reports of ectopic salivary tissue in the anterior mandible [6, 7]. If ectopic salivary tissue can involve the mandible, it should also be able to involve middle ear structures, given their common embryologic origin.
Buckmiller et al. reviewed 25 cases of middle ear choristoma and suggested that there may be a ‘syndrome’ associated with middle ear choristoma. They report associated abnormalities of the first and second branchial arches (including pre-auricular pits, ossicular abnormalities, and absence of the tensor tympani tendon) and of the otic capsule (such as cochlear aplasia). This ‘syndromic’ view of middle ear choristoma is corroborated by our report. Our patient has malformed ipsilateral ossicles, a malformed epitympanum, absence of the tensor tympani tendon, and the remote history of ‘skin tag’ excision from the ipsilateral ear.
We present a case of salivary middle ear choristoma. This patient had multiple other abnormalities of the ear, including malformed ossicles, tegmen tympani defect and a malformed epitympanum. Middle ear salivary choristoma is a rare, but not unheard of, entity. It is usually diagnosed on pathology, as it can be clinically confused with the much more common cholesteatoma. Frequently, this diagnosis is associated with a variety of other external, middle, and inner ear abnormalities.
CONFLICT OF INTEREST STATEMENT
The authors declare that there is no conflict of interest regarding the publication of this paper.

{kind=link}
{kind=link}
{kind=link}