





Abstract
Anomalies of the appendix are extremely rare, with a reported incidence of 0.004 to 0.009. Due to the wide range of variations, failing to recognize these anomalies may lead to failure of treatment and complications. We report a case of a 21-year-old female patient who presented to the Emergency Department with a clinical picture of acute appendicitis. After performing the proper laboratory and radiological tests, a decision was made to do a laparoscopic appendectomy which revealed a partially duplicated ‘bifid’ vermiform appendix with features of acute appendicitis.
INTRODUCTION
Duplication of the appendix is a rare congenital anomaly with an incidence rate ranging from 0.004 to 0.0009 [1]. Due to the rarity of these anomalies, correct identification is important in order to avoid any harmful medico-legal consequences associated with missing a second appendix during surgery.
CASE REPORT
A 21-year-old female patient presented to the emergency department complaining of abdominal pain that started 12 hours ago. The pain started gradually as a stabbing pain around the umbilicus with eventual shift towards the right iliac fossa. She had loss of appetite and persistent nausea that was occasionally accompanied by vomiting. She denied any change in bowel habit or history of similar pain in the past. She had regular periods with no gynecological complaint. The patient was otherwise healthy with no previous past medical or surgical history.
On physical examination, the patient looked ill and tired. She had tachycardia but was afebrile. Examination of the abdomen revealed sever localized tenderness at the right iliac fossa, no guarding or rigidity. Blood tests were within normal values.
Abdominal ultrasonography was performed and revealed a distended appendix measuring 10 mm with appendicolith seen at the base and increased echogenicity surrounding fatty planes. A diagnosis of acute appendicitis was made based on the Ultrasonography findings and the patient was planned to undergo laparoscopic appendectomy. Initial diagnostic laparoscopy showed a small amount of free fluid in the abdomen and a swollen and slightly erythematous partially duplicated ‘bifid’ appendix Fig. 1. A traditional laparoscopic appendectomy was performed by dissecting the mesoappendix and ligating the base of the appendix. The appendix was then exteriorized and sent for histopathology which showed acute inflammation in the two lumens that were lined by appendiceal mucosa and two layers of musculature due to fecalith impaction which is consistent with true duplication of the appendix Fig. 2.
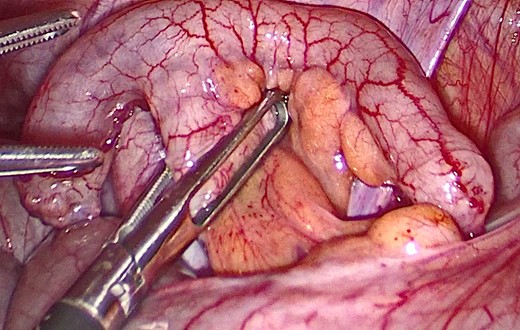
Laparoscopic view of the bifid appendix.

Gross view of the bifid appendix.
The post-operative course was uneventful and the patient had a full recovery without complications and was discharged on the second postoperative day.
DISCUSSION
Anatomical anomalies of the vermiform appendix are often asymptomatic and their discovery is done intraoperatively the majority of the time. However correctly identifying these anomalies in the setting of acute appendicitis is very important due to the life threatening consequences associated with the failure of treatment and they can often represents a manifestation of more complex developmental intestinal, genitourinary or vertebral abnormalities specially in children.
To better understand these anomalies, we should study the embryology of the normal appendix. During the fifth week of gestation, the appendix originates from a bud at the junction of the small and large bowel and undergoes rapid growth into a pouch. It is only after the 20th week of gestation that the proximal end of this pouch starts growing differentially to give rise to the true cecum that continues to develop into infancy [2]. Due to the common origin of the appendix and the cecum, true appendiceal duplication is only confirmed when histopathology shows that both specimens are lined with appendiceal mucosa and coated with two layers of musculature which was present in our case [3]. Although normal embryogenesis of appendix is known, the pathogenesis of its duplication is unclear.
The first to publish a clinical report describing appendiceal duplication was Picoli in 1892. However, with more than one hundred cases reported in the literature to date, multiple classifications have been proposed throughout the years to classify these anomalies and provide the proper management for each variant. Nowadays, the most widely accepted classification is the ‘Cave–Wallbridge’ classification which was first proposed by Cave in 1936 and later modified by C. Waugh and Wallbridge in 1963 [4]. It was later modified again by Biermann in 1993 [5].
In the ‘Cave–Wallbridge’ classification, anatomical variation of the appendix were grouped into three major categories based on the appendicular localization, namely category A, B and C, with category B and C being further divided into more subgroups.
The first category in the ‘Cave–Wallbridge’ classification, Category A, describes the presence of a single cecum that gives rise to a completely or partially duplicated appendix with a common base.
However, when two completely separated appendices are present, they are either classified as a type B1 ‘avian type’ when both appendices are located symmetrically on either sides of the ileocecal valve or a type B2 ‘tenia coli type’ when one appendix arises from the cecum normally while the other arises from the anterior tinea coli muscles at a variable distance from the first.
The last, and also the rarest, variant is the type C category which corresponds to the presence of two separate cecums each with its own appendix along with other more rare anomalies such as horseshoe and triple appendices.
In 2017, Nageswaran et al. published a comprehensive review of more than 140 cases of appendiceal anomalies published in the English and non-English literature [6]. According to Nageswaran et al., type B2 was by far the most common with 73(59%) cases Table 1.
The modified Cave–Wallbridge classification and the frequency of each type of appendiceal duplication.
| Category of anatomical variation | Frequency n(%)* |
|---|---|
| CW Type | 22 (18) |
| CW Type B | 73 (59) |
| Type B1 | 8 (6) |
| Type B2 | 46 (37) |
| Type B unable to classify further | 19 (15) |
| CW Type C | 10 (8) |
| Horseshoe | 6 (5) |
| Triple | 2 (2) |
| A Miscellaneous configuration not fitting any category | 6 (5) |
As reported by Nageswaran et al.
Since the Nageswaran et al. review, only four cases of appendiceal anomalies have been reported in the literature other than our case.
The first of these was published by Triki et al. [7] in 2017, when they reported on a case of a 35-year-old female who presented with right iliac fossa pain. Preoperative workup leads to a diagnosis of complicated acute appendicitis. During surgery, a localized peritonitis in relation to two phlegmonous appendages linked by a common base was identified. Histological examination confirmed the duplicated and phlegmonous appearance of the appendix consistent with a Cave–Wallbridge category A.
Ayoub et al. [8] also published an interesting case of a 30-year-old female who underwent open appendectomy for acute appendicitis. During surgery, two appendices on either side of the ileocecal valve were identified with acute appendicitis in only one of them which is consistent with a Cave–Wallbridge category B1 duplication. Both appendices were resected to avoid any future diagnostic confusion.
Lieu et al. [9] was the last to report a case of duplicated appendix in a 22-year-old man who was found to have a horseshoe appendix with the two bases forming a circle, each communicating with the cecum.
CONCLUSION
Although appendiceal duplication is rare, it should not be ignored by the surgeon as it may lead to serious ethical and legal issues if not recognized. Surgeons should always be aware of this possibility even in a patient with a history of a previous appendectomy. To the best of our knowledge, this case is the first to be reported in Jordan.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
The authors received no financial support for the research and/or authorship of this article.

{kind=link}
{kind=link}