





Abstract
Irretrievable rectal foreign bodies can cause significant distress and generally require emergency medical attention. While smaller objects can often be removed trans-anally, larger objects typically require more invasive intervention. Here, we report the case of a 57-year-old man who had previously presented to the emergency department with a baseball lodged in the rectosigmoid that required a laparotomy. One year later, he represented with a significantly larger object also affixed in the rectosigmoid. Exploratory laparotomy revealed an edematous, inflamed bowel with extensive adhesions from the pervious surgery. Given the degree of tissue damage and large size of the object, the decision was made to perform a Hartmann’s procedure. The object, an 11 × 10 cm rubber chew toy, was successfully removed and the patient was referred to the appropriate mental health professionals during follow-up.
INTRODUCTION
Reports of medically concerning rectal foreign bodies date back to the 16th century [1]. While relatively uncommon, the number of patients presenting to emergent care with irretrievable rectal foreign bodies appears to be increasing [2]. Though smaller, ingested objects can occasionally become lodged in the rectum, large objects are almost always inserted trans-anally. Rarely, large objects can be introduced for diagnostic/therapeutic purposes, or for criminal reasons such as assault or concealing illicit drugs. However, far more often, these objects are introduced trans-anally for sexual purposes [2, 3]. In fact, these account for over 75% of cases, and disproportionately affects men [2, 4].
Irretrievable foreign bodies can be alarming as they typically cause pain, obstruction, and/or bleeding. Further, they can cause life-threatening complications if not properly and promptly managed. Such complications include permanent rectal trauma, peritonitis, and bowel perforation [3]. Fortunately, there are a variety of both invasive and non-invasive surgical techniques that can aid in safely removing rectal foreign bodies and minimizing life-threatening sequelae. Here, we present the case of a patient with a long-standing history of rectal foreign bodies, two of which required surgical intervention. At this most recent visit, we found an 11 × 10 cm rubber chew toy lodged in the rectosigmoid, ultimately requiring Hartmann’s colostomy.
CASE PRESENTATION
A 57-year-old man presented to the emergency department complaining of severe rectal pain. He reported inserting a foreign object into his anus earlier that day that he was unable to remove. The patient was clinically obstructed, but denied nausea, vomiting, fever, chills, or abdominal pain. On physical exam, he was afebrile, hypertensive, and tachycardic. Additionally, gross blood was appreciated at the rectum and his abdomen was mildly distended. Digital rectal exam revealed a large, firm, rubber object approximately 9 cm from the anal verge. Labs were ordered including a complete blood count, comprehensive metabolic panel, and coagulation studies, all of which were unremarkable apart from a mild leukocytosis (11.8).
His medical history was significant for a previous irretrievable rectal foreign body 1 year earlier. This required transabdominal extraction, which revealed a baseball measuring 7.5 cm in diameter. At this most recent visit, an abdominal X-ray was ordered showing a large, mixed low and high-density foreign body fixed in the rectosigmoid colon (Fig. 1). Several attempts were made to remove the new object trans-anally, all of which were unsuccessful. At this time, the surgical team decided to perform exploratory laparotomy. Due to the severe inflammation and edema of the rectosigmoid (Fig. 2), as well as adhesions secondary to the previous abdominal surgery, a Hartmann’s procedure with creation of end sigmoidostomy was required. The object, a rubber chew toy, was successfully removed and measured 11 cm in length and 10 cm in diameter (Figs 3 and 4). The patient’s post-operative course was complicated by a prolonged ileus. He was discharged home on post-operative day 10 and recovered appropriately. Colostomy reversal was discussed and he was followed as an outpatient.

Abdominal X ray showing a large, mixed low and high-density foreign body in the rectosigmoid.
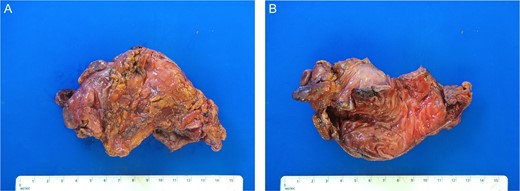
Gross pathology photos of surgical specimen. (A) External surface of the resected bowel. (B) Internal surface of the resected bowel.
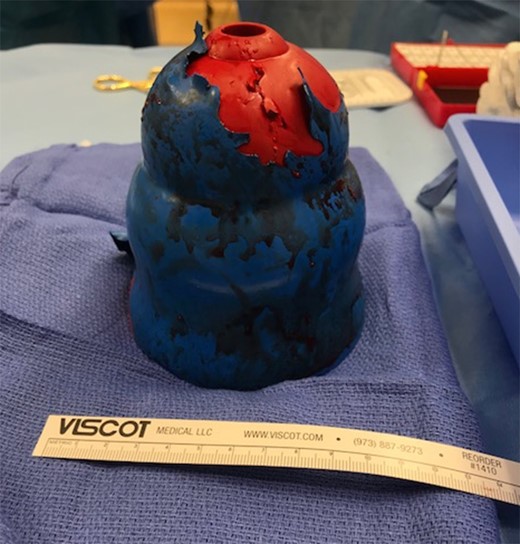
Intraoperative photo of the rectal foreign object.
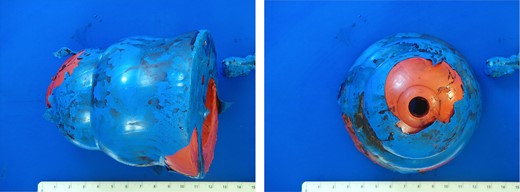
Postoperative photos of the rectal foreign object.
DISCUSSION
Rectal foreign bodies can pose a significant clinical challenge. Typically, patients will present with abdominal pain or obstruction. While diagnosis is often straightforward, patients may be hesitant or unwilling to share the etiology of their symptoms due to embarrassment. It is therefore imperative for clinicians to remain supportive and non-judgmental when taking a history in order to expedite diagnosis [5]. Once a rectal foreign body is confirmed, the first priority is to identify potential peritonitis via abdominal exam. Next, a digital rectal exam should be performed in order to assess the location, shape, and size of the object [6]. Care providers must also examine the anal sphincter muscles in order to better characterize a potential injury and risk for incontinence.
Radiographic imaging of the abdomen should be obtained quickly, as this can aid in identifying the size and location of the object, as well as any obvious bowel perforation. While laboratory studies are generally unhelpful in diagnosing a rectal foreign body, they should also be performed to assist in the diagnosis of more serious sequelae. Notably, an elevated white blood cell count and/or lactic acidosis can be concerning for perforation, suggesting the need for emergent laparotomy [5].
When a rectal object cannot be retrieved via digital rectal or bimanual examination, local/spinal anesthesia or conscious sedation can often reduce sphincter tone and make extraction possible. However, when these techniques fail, determining the correct course of action can be difficult. The most common approach is attempting to grasp the object with polypectomy snares during endoscopy [7]. Alternative methods include inflating a Foley catheter or achalasia balloon into the rectosigmoid proximal to the object [7, 8]. If these approaches are also unsuccessful, surgery may be necessary.
During surgery, it is important to evaluate the bowel for hematomas, lacerations, or devascularized segments, as these may mandate resection [5]. If not observed, the first approach should be to ‘milk down’ the object and extract trans-anally [9]. Should this approach fail, a colotomy is likely necessary. Regardless of the approach used, it is crucial to conduct immediate endoscopic evaluation of the bowel after removing the object to ensure there is no additional injury [10]. It is also crucial to provide additional supportive care, particularly with respect to mental health. Our patient, having presented with the same complaint previously, failed to receive proper psychological evaluation at that time. It is therefore essential to refer patients to the appropriate mental health specialists for counseling, particularly in cases with repeated incidents or those involving assault [5].
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts to disclose.
FINANCIAL INFORMATION
D.R. Principe is supported by the National Cancer Institute of the National Institutes of Health under Award Number F30CA236031.
REFERENCES
Author notes
These authors contributed equally to this work and serve as joint first authors.

{kind=link}
{kind=link}
{kind=link}
{kind=link}