





Abstract
Barotrauma to the colon and rectum is well documented, most commonly due to endoscopic complications. Here, we describe the unique case of a 56-year-old male presenting with peritonitis after self induced barotrauma to his colon following an attempt to alleviate 4-day obstipation with a toilet plunger. Exploratory laparotomy revealed a perforated and gangrenous right colon, which was promptly treated with an open right hemicolectomy and end-loop Prasad ileocolostomy. To our knowledge, this represents the first case of its kind and highlights the distinct pathology for colorectal barotrauma depending on the underlying mechanism of injury.
INTRODUCTION
Injury of the large intestine due to barotrauma has been well documented, with the earliest reported case in 1904 [1]. Most commonly, barotrauma occurs as the result of endoscopy, however, several additional etiologies have been reported, including the transanal introduction of air pressure from air jets and water-soap enemas [2]. Here, we describe a unique case of gradual, trans-anal barotrauma resulting in cecal perforation as a result of a toilet plunger used to relieve severe constipation.
CASE REPORT
A 56-year-old male with history of bipolar disorder, alcoholism and diverticulosis presented to the emergency room complaining of abdominal pain for 14 hours, which he described as severe, non-radiating, and diffuse. Prior to the onset of pain, the patient described obstipation for 4 days, which he attempted to relieve by introducing air to his rectum using a toilet plunger. On physical exam, the patient was hypothermic, tachycardic, and normotensive. His abdomen was distended with peritonitis, and lab work was only significant for lactic acidosis.
A computed tomography (CT) scan of the abdomen and pelvis showed a large fluid collection in the retroperitoneum abutting the right colon and duodenum, tracking into the right paracolic gutter, with associated pneumoperitoneum as well as free air within the retroperitoneum and mediastinum (Fig. 1).
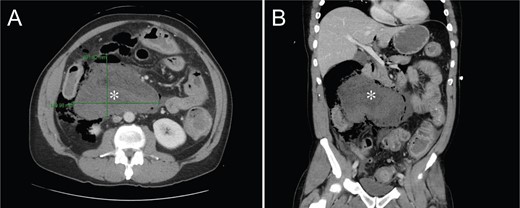
CT of the abdomen and pelvis showing a 10.2 × 14.1 × 14.1 cm collection of stool, fluid and gas along the right colon.
An exploratory laparotomy was performed through a midline incision. The right colon was gangrenous and perforated into the mesentery (Fig. 2), which contained a large amount of feces. A right hemicolectomy with end-loop Prasad ileocolostomy with abdominal lavage were performed. Tissues were sent to pathology, which confirmed the presence of a cecal perforation with acute serositis and pericolonic abscess formation. No diverticula, obstruction or polyps were identified.

Gross Pathology of Surgical Specimen. (A) External surface of the resected bowel. (B) Internal surface of the resected bowel at low magnification. (C) Internal surface of the resected bowel at high magnification. Yellow arrows indicate cecal perforation.
The patient’s case was complicated by aspiration on induction of anesthesia. As a result, his post-operative course was remarkable for aspiration pneumonia resulting in respiratory failure requiring tracheostomy, as well as dysphagia requiring percutaneous gastrostomy tube placement. He was discharged to an extended care facility on post-operative day 46.
DISCUSSION
While barotrauma to the colon and rectum is well understood, to our knowledge this patient represents the first case of barotrauma due to a toilet plunger. Due to the difference in etiology, our patient displayed atypical injury of the cecum, whereas most cases affect the distal colon, sigmoid, or rectum [2]. This was most likely the result of the gradual introduction of pressure by the plunger. Contrastingly, the rapid introduction of air by an air jet or high-pressure blowgun has a sudden burst pressure that places the recto sigmoid at higher risk for perforation [3].
Endoscopy is the most common cause of injury from gradual barotrauma, though most colonoscopy-associated perforations are found in the sigmoid [4], which can be explained through several mechanisms. During colonoscopy, the anatomical bend of the sigmoid creates a closed loop obstruction in which air pressure accumulates, making this area highly susceptible to barotrauma [5]. The sigmoid colon’s angularity also predisposes the area to mechanical perforation, as it is a difficult location to navigate during endoscopy [5]. Finally, the sigmoid is a common site for therapeutic intervention e.g. polypectomy, electrocaudary, etc., nearly all of which have an inherent risk of perforation [6].
The cecal injury observed in our patient is rather uncommon, and can most likely be explained by the Law of Laplace. This law states that the tension in the walls of a container is dependent on both the pressure of its contents and its radius [7]. In other words, as the cecum has the largest diameter in the colon, it requires the least amount of pressure to distend [5]. This has been substantiated in cadaver experiments, in which it was determined that a pressure of 81 mmHg is required to rupture in cecum, whereas 169 mmHg is necessary to rupture the sigmoid [8]. In this case, the use of an average sized plunger can theoretically introduce nearly 650 cm3 of compressed air with each complete seal. Should the patient have reaffixed the plunger multiple times, even with a partial introduction of trapped air or an incomplete seal, the pressures generated would be more than sufficient to cause the injury observed.
Still, as this is an incredibly unlikely cause for cecal perforation, we also questioned the patient regarding several additional risk factors, all of which he denied. These include a history of inflammatory bowel disease or cancer, recent colonoscopy, or the use of medications such as Ipilimumab that have been linked to bowel perforation [9]. These pertinent negatives further suggest that the plunger-associated barotrauma was indeed sufficient to perforate an otherwise healthy cecum.
The management of intestinal barotrauma/perforation depends largely on degree of injury and timing of presentation. Treatment can range from simple rectal tube decompression to bowel resection. As our patient presented with feculent peritonitis and gangrenous bowel, an exploratory laparotomy and ostomy were required. Reversal of the ostomy will depend on patient recovery, as well as subsequent imaging and/or endoscopic evaluation.
CONFLICT OF INTEREST STATEMENT
None declared.
CONFLICT OF INTEREST DISCLOSURE
The authors have no conflicts to disclose.
FINANCIAL INFORMATION
D.R. Principe is supported by the National Cancer Institute of the National Institutes of Health under Award Number F30CA236031.
REFERENCES
Author notes
Jonathan Rubin and Daniel R Principe authors contributed equally and serve as joint first authors.

{kind=link}
{kind=link}