





Abstract
The incidence of internal hernias is rare (0.2–0.9%). The prevalence of intestinal obstruction for an internal hernia is low (0.5–5%), however if strangulation is present the overall mortality is higher than 50%. There are multiple places where an internal hernia may be localized, with transmesenteric: transmesocolic (8%) and transomental (1–4%) as the rarest. We report a series of two cases (men with 40 years-old and women with 92 years old) of volvulus of colon sigmoid in a strangulated transverse and descendent transmesocolic hernia, with one case associated also to a transomental hernia. Both patients were submitted to a Hartmann procedure and on follow-up remained free of complains. In conclusion, transmesenteric internal hernia should be included as diagnosis hypothesis for intestinal occlusion and if the diagnosis is made, the patient should be submitted to emergency surgery due to high rates of complications, high morbidity and mortality.
INTRODUCTION
Internal hernia is a protrusion of an intraperitoneal content through an anatomical or pathological opening of peritoneal cavity, leading to impaction within another compartment of the otherwise intact cavity [1, 2]. The incidence of internal hernias is rare (0.2–0.9%) [1]. The prevalence of intestinal obstruction for an internal hernia is low (0.5–5%), however if strangulation is present the overall mortality is higher than 50% [1].
There are multiple places where an internal hernia may be localized, being paraduodenal (53%) the most common localization and the transmesocolic (8%) and transomental (1–4%) the rarest [2]. Internal hernias can be congenital or acquired [2]. Transmesenteric internal hernias consist of two types: transmesocolic and transomental [3]. The most common risk factors for acquired internal transmesocolic hernias are previous surgery, history of trauma or peritoneal infection [1]. Congenital transmesenteric hernias are more common on children [1].
CASE REPORTS
We report a series of two cases.
Case 1: A 40-year-old men, without previous abdominal surgery or history of abdominal trauma or peritoneal infections was admitted to the emergency department with generalized abdominal pain, nausea and vomiting. Physical exam revealed a distended abdomen, with pain in the epigastrium without tenderness. Laboratory investigation on admission was normal. Abdominal X-ray revealed a marked sigmoid colon distension suggestive of a colonic volvulus. A colonoscopy was conducted and revealed necrosis of the colon sigmoid apparently form a colonic volvulus. Abdominal-pelvic computerized tomography(CT) was conducted and a colonic volvulus associated with a transmesocolic hernia with transmural necrosis of the colon sigmoid was identified (Fig. 1). The patient was proposed to laparotomy during which a volvulus of sigmoid colon with transmural necrosis in a strangulated descendent transmesocolic hernia was identified. A Hartmann procedure was conducted and the patient was discharged at sixth post-operative day. At 2 year follow-up consultation, the patient remained free of complains, with the intestinal transit re-established.

Abdominal-pelvic CT—coronal plane: colonic volvulus associated with a transmesocolic hernia with transmural necrosis of the colon sigmoid.
Case 2: A 92-year-old women, without previous abdominal surgery or history of abdominal trauma or peritoneal infections was admitted to the emergency department with generalized abdominal pain. Physical exam revealed markedly distended abdomen with generalized abdominal pain with tenderness. Laboratory investigation on admission: white cell count of 30.200/mm3 with 84.7% neutrophils, protein C reactive of 13.6 mg/dL and lactates of 2.17 mmol/l. Abdominal X-ray showed a marked colonic enlargement. Abdominal-pelvic CT identified a colonic volvulus associated with a transmesocolic hernia with transmural necrosis of the colon sigmoid (Figs 2 and 3). The patient was proposed to laparotomy during which a volvulus of colon sigmoid with transmural necrosis in a strangulated transverse transmesocolic and transomental (great omentum) hernia was identified (Figs 4 and 5). A Hartmann procedure was conducted and the patient was discharged at fifth post-operative day. At 3 months follow-up consultation, the patient remained free of complains.
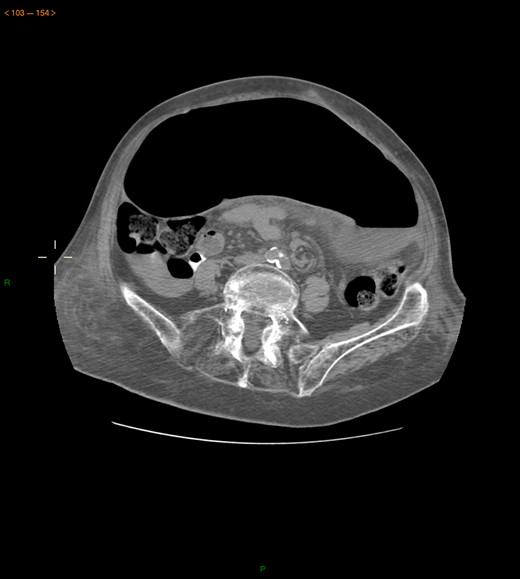
Abdominal-pelvic CT—transverse plane: colonic volvulus associated with a transmesocolic hernia with transmural necrosis of the colon sigmoid.

Abdominal-pelvic CT—coronal plane: colonic volvulus associated with a transmesocolic hernia with transmural necrosis of the colon sigmoid.
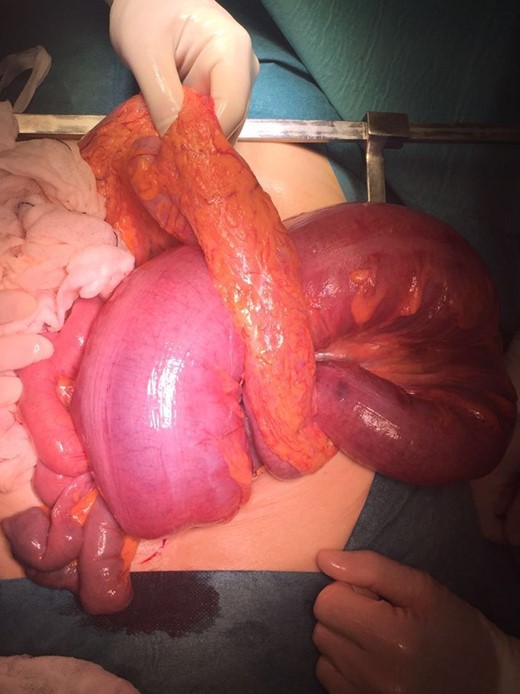
Intraoperative image: colon sigmoid with transmural necrosis in a strangulated transverse transmesocolic and transomental (great omentum) hernia.
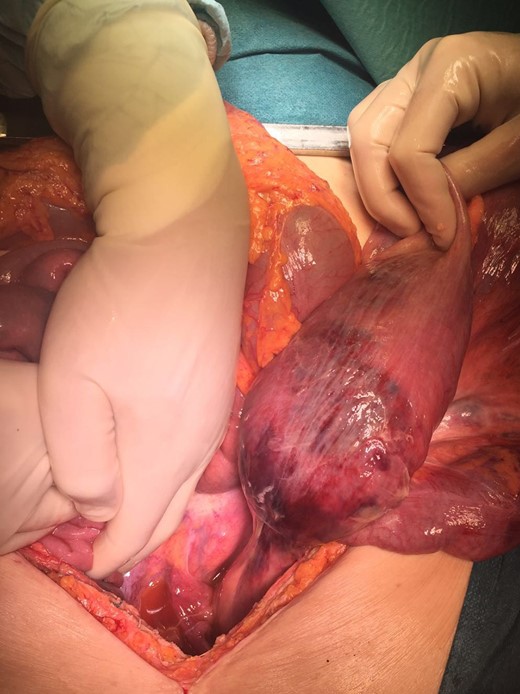
Intraoperative image: volvulus of colon sigmoid with transmural necrosis in a strangulated transverse transmesocolic and transomental (great omentum) hernia.
DISCUSSION
Transmesenteric hernias include two types: transmesocolic and transomental, both of which are quite rare [1, 3]. In adults, the main etiology of this type of hernia are previous abdominal surgery, history of trauma or history of peritoneal infections [1, 2]. Congenital origin in adults are extremely rare and only few cases where published in the literature [1]. Usually the defect in the mesocolon is a very large avascular space [4]. Transomental hernia usually occur after re-entry into the great peritoneal cavity via foramen of Winslow, gastrohepatic ligament or gastrocolic ligament after a transmesocolic hernia trough the transverse mesocolon [4]. To our knowledge, congenital transmesenteric hernias published in the literature were only with small bowel, with the majority within the mesocolon sigmoid (60%) [1–6]. In contrast, our series describes two cases of strangulated tramsmesocolic hernias with colon sigmoid, and one of them with transomental hernia associated.
The preoperative diagnosis of transmesenteric hernias preoperative is quite hard, however abdominal CT might help: engorgement of the mesenteric vascular structures; abnormal right or left displacement of the colon; dilation of prestenotic small bowel loops or colon; absence of intraluminal contrast progression associated with distension content [1, 2, 5]. However, the identification of the type of internal hernia base on clinical and radiologic findings is often impossible [2]. Suspicion of a congenital transmesenteric hernia should be present in adults of all ages, if the risk factors are not present as a cause of intestinal occlusion.
Compared to other subtypes of internal hernias, transmesocolic more often develop complications such as volvulus(30%), strangulation, ischemia(40%) and perforation [2, 5]. In our series, both cases were associated with volvulus and strangulation. Unfortunately, as our series document, the majority of times there are intestinal necrosis, even if the laboratory analysis is relative normal, with the need of intestinal resection [1, 2, 5]. Our series also demonstrate that if the colon is strangulated, the majority of times is colon sigmoid, possible due to a more redundant mesocolon.
In conclusion, transmesenteric hernia should be always included as diagnosis hypothesis for intestinal occlusion and if the diagnosis is made, the patient should be submitted to emergency surgery due to high rates of complications, high morbidity and mortality.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}