





Abstract
Acute appendicitis is one of the top differential diagnoses of right lower quadrant pain in the emergency department. There are many other conditions that may mimic appendicitis such as diverticulitis, colitis and gynecological conditions. We report a rare diagnosis of a patient who presents with characteristic clinical and laboratory features of appendicitis with severe sepsis, but later showed acute pyelonephritis of a malrotated right ectopic kidney on computer tomography. An ectopic kidney is very rare with an incidence of 1 in 3000. It is usually asymptomatic, although it may also associate with obstruction, infection and urolithiasis. This case report raises the importance of early recognition of the correct diagnosis using imaging in appropriate clinical settings, and prompt antibiotic treatment can avoid unnecessary surgical intervention, preserve renal function and prevent a life-threatening catastrophe.
INTRODUCTION
Abdominal pain is one of the common presentations to the emergency department. When a patient presents with right lower quadrant abdominal pain and fever, acute appendicitis is one of the most likely differentials, along with other conditions that may mimic acute appendicitis such as diverticulitis, colitis and gynecological conditions. An ectopic kidney located in the right lower abdomen with acute pyelonephritis is a very rare presentation and diagnosis can be challenging [1]. Misdiagnosis of appendicitis leads to unnecessary operations and a delay in the diagnosis of acute pyelonephritis can lead to renal scarring, which in turn may be associated with hypertension and chronic renal failure [2]. We report a rare case of a lady who presented with clinical appendicitis who had a malrotated right ectopic kidney with severe pyelonephritis and summaries the related literature.
CASE REPORT
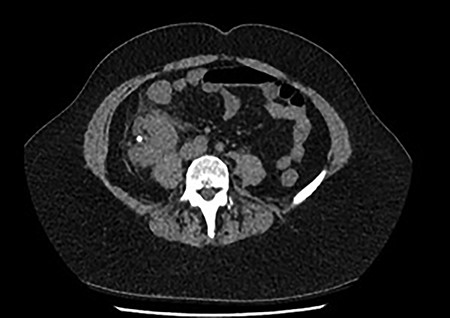
A 60-year-old lady presented to the emergency department with a 1-day history of migratory right lower quadrant pain, diarrhea and associated fevers and rigors. She had a background history of previous diverticulitis and hypertension. On examination, she was shocked with a blood pressure of 86/52, was borderline tachycardiac at 95 bpm, she was tender in the right lower quadrant with guarding and laboratory tests showed acute kidney injury (AKI) with an eGFR of 37 ml/min (previously normal renal function) and a white cell count of 32.9 (109/L). She was referred to the surgical team with a clinical diagnosis of acute appendicitis with an Alvarado score of nine [3]. On further investigation, her urine microscopy showed >500 leucocytes. Because of her age, highly positive urine microscopy (MCS) and AKI, a non-contrast computer tomography (CT) was performed, which showed a malrotated right ectopic kidney with perinephric stranding and a non-obstructing 6 mm calculus in renal pelvis (Fig. 1).

Coronal and transverse CT showing a malrotated right kidney with a non-obstructive calculus and marked perinephric stranding. This ectopic kidney also has an abnormal axis, facing anterolaterally.
Coronal and transverse CT showing a malrotated right kidney with a non-obstructive calculus and marked perinephric stranding. This ectopic kidney also has an abnormal axis, facing anterolaterally.
She was treated with ampicillin and a reduced dose of gentamicin given her AKI. Because of persisting shock, this patient was admitted to the intensive care unit (ICU) for inotropic support. Subsequently, both the urine and blood culture grew Escherichia coli. A repeat CT with contrast was performed due to persisting high fevers and severe right lower quadrant pain, which showed an early renal abscess (Fig. 2). Because of ongoing sepsis and absence of urology service in our hospital, the patient was transferred to another hospital where a urology service was available. She subsequently had insertion of a ureteric stent. The patient continued to improve post stent insertion and discharged when clinically well. She had removal of stone and ureteric stent 6 weeks later.
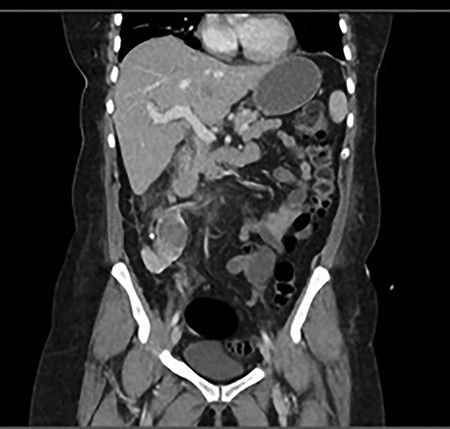
Progress CT showed worsening of perinephric inflammatory stranding and low-density area at the interpolar and upper pole of the right kidney representing an early renal abscess.
DISCUSSION
An ectopic kidney is very rare with an incidence of 1 in 3000 [4]. During normal embryological development, there is cephalic migration of the kidneys to their normal retroperitoneal location and an ectopic location is a result of arrested ascent. Ectopic kidneys can be found in the pelvis, iliac, abdominal, thoracic or contralateral positions [5]. Factors that may prevent the orderly movement of kidneys include ureteral bud mal-development, defective metanephric tissue that fails to induce ascent, genetic abnormalities, teratogens and maternal illnesses or teratogenic causes [4].
Over half of ectopic kidneys have a dilated collecting system with hydronephrosis as a result of the malrotation alone, high grade vesicoureteral reflux or obstruction at the level of the ureteropelvic or ureterovesical junction. Most individuals with ectopic kidneys are asymptomatic, however, common complications such as obstruction, infection and urolithiasis may occur [2]. This is due to an anteriorly placed pelvis or an anomalous vasculature that partially blocks one of the major calyces or the upper ureter, which make it prone to have infections and stone formation [4]. The patient described in this case report had urolithiasis and pyelonephritis. The blood supply of an ectopic kidney varies, with the possibility of more than one aberrant artery or arteries that originates from the aorta, common iliac, external iliac or the inferior mesenteric artery [6]. Furthermore, there may be an increased risk of injury from blunt abdominal trauma because the low-lying kidney is not protected by the rib cage [7].
An ectopic kidney is associated with a number of congenital defects especially genital anomalies. In women, congenital defects include unicornuate or bicornuate uterus with atresia of one horn, a rudimentary or absent uterus and proximal and/or distal vagina, and duplication of the vagina. Whereas in male patients, 10–20% have a recognizable associated genital defects including undescended testes, duplication of the urethra, and hypospadias are also common [7].
An ectopic kidney with acute pyelonephritis mimicking acute appendicitis has been rarely described in the literature. Symptoms and signs of pyelonephritis in a pelvic kidney may mimic appendicitis. Patients with appendicitis commonly present with right lower quadrant pain, anorexia, fever, nausea and vomiting which are also common symptoms in pyelonephritis [2]. Furthermore, patients with appendicitis of a pelvic appendix in close proximity to the bladder can have dysuria and positive urine microscopy. Imaging techniques such as ultrasound and CT have been commonly used in assisting the diagnosis of adults presenting with abdominal pain. CT has a sensitivity and specificity for diagnosis in adults of 94% and 94%, respectively [1].
This case report highlights the importance of performing imaging on adults with suspected acute appendicitis prior to surgical intervention, especially in the age group where appendicitis is less likely and in the setting of a significant urine culture result. It is important to raise awareness of the possibility of an ectopic kidney with pyelonephritis that may mimic appendicitis. Accurate differentiation between these two conditions is crucial as it can avoid unnecessary surgical intervention, improve patient care and outcome.
REFERENCES

{kind=link}
{kind=link}
{kind=link}