





Abstract
Giant coronary artery aneurysms are an infrequent finding. They are typically discovered incidentally, rarely presenting with any symptoms. We present the case of a 72-year-old gentleman who presented with an ST elevated myocardial infarction. On investigation, the gentleman was found to have a giant right coronary artery aneurysm which was partially filled with a fresh thrombus. The thrombus occluded the RCA, triggering the myocardial infarction which leads to this gentleman’s presentation to a tertiary cardiac centre. The gentleman underwent a successful resection of the aneurysm and coronary artery bypass graft over the RCA lesion with a saphenous vein conduit. This gentleman has since been discharged from hospital after an uncomplicated postoperative course.
INTRODUCTION
Giant coronary artery aneurysms are defined as aneurysms of the coronary arteries with a diameter greater than 2 cm [1]. Coronary artery aneurysms in children and adolescents are often associated with Kawasaki’s disease [2]. There are numerous potential causes in adults, including atherosclerosis, stent implantation, vasculitis, autoimmune diseases, familial hypercholesterolaemia and blunt force chest injury [3].
We present the case of a 72-year-old gentleman with a giant right coronary artery (RCA) aneurysm.
CASE REPORT
A 72-year-old gentleman presented to the ambulance service with central non-radiating chest tightness associated with nausea and sweating. Electrocardiogram (ECG) showed inferior ST-elevation with reciprocal changes in V1–V3. The gentleman was admitted to a tertiary cardiac centre for primary percutaneous coronary intervention.
The patient has previous diagnoses of hypertension and benign prostatic hyperplasia. He had no previous cardiac events or anginal episodes.
Echocardiogram was performed, showing hypokinesia of the inferior wall. This finding is consistent with an inferior myocardial infarction, as was suggested by the ECG. During the echo, the patient went into a shockable ventricular fibrillation rhythm several times and required defibrillation up to 12 times. A bedside echo was subsequently performed revealing a suspicious looking structure around the right atrium and right ventricle.
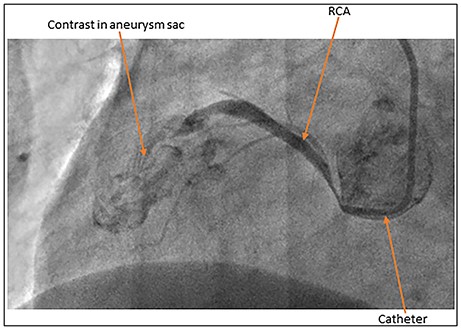
Coronary artery angiogram showing extravasation of contrast into the aneurysm sac.
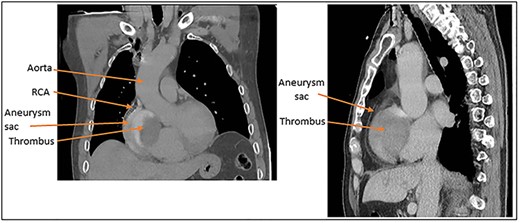
(A) Coronal and (B) sagittal CT images of the large aneurysm sitting over the right side of the heart and the thrombus within the aneurysm.
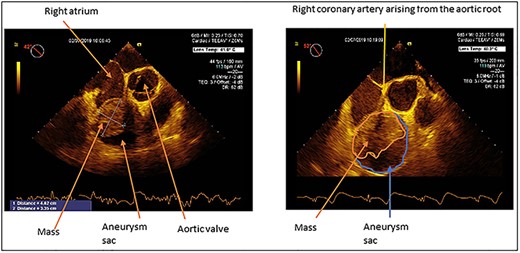
Transoesophageal echo demonstrating RCA aneurysm with a mass partially filling the aneurysm sac. The size of the mass is 4.62 by 3.35 cm. The proximal RCA is seen originating from the aortic root.
Coronary angiogram demonstrated a normal left main stem, disease in the mid-left anterior descending artery and a minor atheroma in the left circumflex artery. The RCA was seen to be filling only to the mid-segment, as shown in Fig. 1, after which the contrast extravasated suggesting a possible aneurysm. No pericardial effusion was seen. Aortogram showed no obvious dissection flap.
The patient then underwent a CT to better visualise the aneurysm, shown in Fig. 2. The RCA was seen to be feeding a localised, well circumscribed, lesion with layering of material suggestive of acute bleeding from the RCA into a possible pre-existing aneurysm.
Transoesophageal echo was performed at the initiation of anaesthesia. This confirmed the dilation of the RCA, and that there was a mass within the dilation, see Fig. 3. The lumen of the RCA was visible running through the mass that partially filled the aneurysm sac.
The patient underwent a successful coronary artery bypass graft and resection of the giant RCA aneurysm under cardiopulmonary bypass via mid-line sternotomy. Intraoperative images can be seen in Fig. 4.
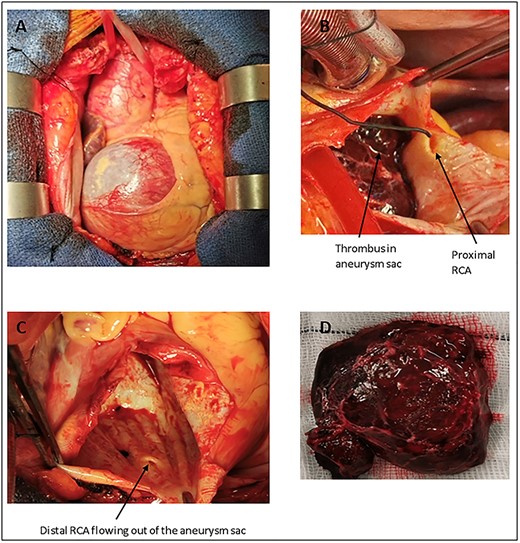
Intraoperative images. Image (A) shows the very dilated RCA visible upon opening the pericardium. Image (B) shows the unaffected portion of the proximal RCA feeding into the aneurysm sac, thrombus can be seen within the sac. Image (C), taken after the thrombus has been removed from the sac, shows the unaffected distal RCA. Image (C) also shows that there are no atherosclerotic plaques or evidence of previous thrombotic events within the aneurysm sac. This finding supports the theory that thrombus formation was an acute event which led to the patient presenting with an STEMI. Image (D) shows the fresh thrombus after it was removed from the aneurysm sac.
A 5.9 by 4.9 cm aneurysm of the RCA was identified. Upon opening, the aneurysm sac was found to be half filled by a fresh clot. The proximal and distal ends of the RCA were identified and transfixed. The sac was closed by continuous suture. The lesion was bypassed with a left saphenous vein graft. The patient made an uneventful recovery and was discharged from the intensive therapy unit on the first postoperative day and home on the sixth postoperative day.
DISCUSSION
A coronary artery aneurysm is defined as a dilation of a discrete area of the artery to more than 1.5 times the diameter of the unaffected adjacent segments [4]. An aneurysm is classed as giant when it exceeds 2 cm in diameter [1]. Giant coronary artery aneurysms are a relatively rare occurrence, with an incidence rate of 0.02–0.2% [5].
From the data collected in Jha et al.’s 2009 literature review, there appears to be a slight predilection for aneurysm formation on the RCA over the left anterior descending (19 RCA, 10 LAD) [1]. A reason for this pattern has not yet been proposed.
This case is of further interest due to the thrombus found within the aneurysm and the potential impact this had on the presentation. The thrombus was soft, indicating it had formed recently within the sac. The RCA, via the posterior descending artery, supplies the inferior wall of the heart in 80% of individuals [6]. This patient presented with an inferior STEMI, which could be attributed to the formation of the thrombus and its subsequent occlusion of the RCA. It is unusual for patients with coronary artery aneurysms to present in this fashion, typically coronary artery aneurysms are an incidental finding [7].
There is a lack of consensus on the best way to manage coronary artery aneurysms due to the lack of reported cases [7]. This adds to the already challenging nature of these patients’ management. As such, an individualised approach is utilised based on the presentation and morphology of each patient’s aneurysm.
Due to the lack of guidance on how best to manage patients with giant coronary artery aneurysms, an individualised approach remains the best option. The reporting of further cases will help to advance the knowledge base of this uncommon condition.

{kind=link}
{kind=link}
{kind=link}
{kind=link}