





Abstract
Laparoscopic cholecystectomies represent one of the most common procedures of General Surgery. Dropped gallstones during laparoscopic cholecystectomy is a rare occurrence but can potentially lead to morbid complications. We present a rare case of a broncho-pleuro-cutaneous fistula in a patient with recurrent abscess formations after an elective laparoscopic cholecystectomy. The fistula formed over 3 years from a gallstone that eroded through the diaphragm, into the pleural space, and eventually into a terminal bronchiole. Bilirubin staining within the fistula tract was confirmed on hematoxylin and eosin staining.
INTRODUCTION
Laparoscopic cholecystectomy has become a common procedure for the general surgeon. It is generally a safe and efficient procedure for a very common problem among Americans. Although there are many known complications of laparoscopic cholecystectomy, perhaps an underappreciated complication is spillage and loss of gallstones. The estimated incidence of lost stones during a laparoscopic cholecystectomy is around 2%, and of those 2%, only 8.5% of the cases are estimated to lead to complications [1]. Between 1991 and 2015, there were little over 250 reported complications of spilled gallstones [2]. The most common complication is intra-abdominal abscesses while rare complications include intra-abdominal abscesses associated with empyema as well as intraluminal bowel erosion leading to mechanical obstruction [3,4]. We report a rare broncho-pleuro-cutaneous fistula caused by a dropped gallstone.
CASE REPORT
A 70-year-old man with a past medical history of hyperlipidemia, osteoarthritis, obesity and cholelithiasis with choledocholithiasis underwent endoscopic retrograde cholangiopancreatography with sphincterotomy and subsequent elective laparoscopic cholecystectomy. The case was complicated by spillage of multiple stones and a dropped small Ligaclip. During the initial operation, all visible stones were removed, and the abdomen washed with copious irrigation. The Ligaclip was not found. The patient recovered well; however, 3 years later, the patient developed right flank erythema. The erythema developed into three discreet abscesses that were incised and drained. The abscesses never healed, and a computerized tomography scan of the abdomen was obtained. It showed a small object consistent with a dropped gallstone located at the confluence of the right flank peritoneum and the adjacent skin. The patient was taken to the operating room (OR) multiple times where two stone fragments were retrieved and eventually a surgical clip was identified and removed. The fistulous tracts that had formed were excised.
The patient recovered well, but <1 month later he noticed an additional draining sinus at the right flank. A fistulogram (Fig. 1) was performed, and it showed a connection between the sinus and a right lower lobe bronchiole. He was taken to the OR for a right thoracotomy with wedge resection of the right lower lobe of the lung and excision of a broncho-pleuro-cutaneous fistula that was found to contain pieces of golden pigmented solid material, which was concluded to be consistent with a gallstone (Fig. 2). This case report presents a patient with an uncommon complication from a dropped gallstone: a broncho-pleuro-cutaneous fistula.

Contrast study of the broncho-pleuro-cutaneous fistula formed by the dropped gallstone
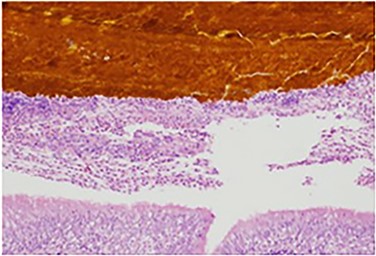
Specimen histology demonstrating bilirubin deposits within the lung parenchyma
DISCUSSION
We are reporting a very rare case of a broncho-pleuro-cutaneous fistula from a dropped gallstone. In another extremely rare case, it has been reported that a patient developed cholelithoptysis after spillage and loss of gallstones from a laparoscopic cholecystectomy [5]. It has been proposed that such phenomenon occurs after abscess formation under the diaphragm cause transdiaphragmatic extensions, in which small stones may pass into the thoracic space, thereby forming bronchopleural fistulas [5]. We propose that our patient had a similar mechanism, in which a migrated stone leads to a nidus for fistula formation, leading to a not yet reported case of a broncho-pleuro-cutaneous fistula from a dropped gallstone.
A broncho-pleuro-cutaneous fistula is a very rare complication from a common general surgery procedure. Spillage of gallstones is a known but avoided complication; and while retrieval of all stones is the ideal objective in these cases, it is not always attainable to collect all stones. In these cases, it is paramount that the operative physician carefully documents such occurrence in the operative report. The radiologist, emergency room physician and surgeon should all give weighted consideration for patients with this known complication if they present in the future with abdominal pain in which the diagnosis points to an acute intra-abdominal process, like an abscess or even an obstruction [6].
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
We have no external funding to disclose. Funding for this case report has come from our institution’s Departments of Cardiothoracic Surgery and General Surgery.
ETHICAL APPROVAL
No ethical approval was required for this case report.
CONSENT
Informed consent was obtained by the subject of this case report.
GUARANTOR
The primary author of this case report, Serena Murphy, will act as the guarantor of this manuscript.
ACKNOWLEDGMENTS
We would like to acknowledge the University of Vermont Medical Center Pathology department for their assistance in this interesting case.
REFERENCES

{kind=link}
{kind=link}