





Abstract
Surgicel® is a commonly used hemostatic agent. We report a case of small bowel obstruction secondary to the prior placement of Surgicel® within the peritoneal cavity, and the radiological diagnosis conundrum and potential prognostic implications this finding has in a patient with a known history of malignancy.
INTRODUCTION
Surgicel® (Ethicon, NJ, USA) is an oxidized regenerated cellulose and a well-known adjunctive hemostatic agent that is used in surgical procedures to assist in the control of bleeding. The cellulosic acid within the product facilitates hemostasis by denaturating blood proteins [1].
This case report highlights the presence of Surgicel® within the peritoneal cavity 2 months following placement causing, firstly, small bowel obstruction and secondly, potential misdiagnosis due to radiological resemblance of Surgicel® and tumors.
CASE REPORT
A 68-year-old male was admitted to hospital for an elective laparoscopy and excisional lymph node biopsy for the investigation of intra-abdominal lymphadenopathy (Fig. 1). An excisional biopsy was performed of an enlarged lymph node in the small bowel mesentery close to the origin of the superior mesenteric artery. Hemostasis was achieved with diathermy and placement of Surgicel® at the site of excised lymph node. The patient had an uncomplicated post-operative stay and was discharged home day one post-operatively. Histopathology of the lymph node confirmed diffuse large B-cell lymphoma. The patient was subsequently commenced on rituximab, cyclophosphamide, doxorubicin, vincristine and prednisolone (R-CHOP) chemotherapy regiment; to which he had a good clinical response.
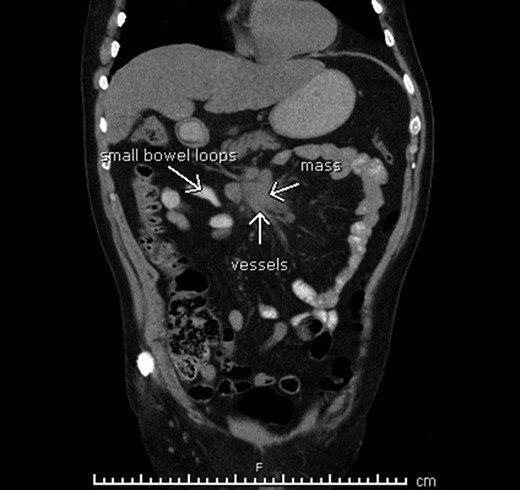
Mesenteric lymphadenopathy found on computerized tomography.
He presented to the emergency department with abdominal pain and fever, 64 days following his initial surgery and 9 days following his last cycle of R-CHOP therapy.
A computed tomography (CT) scan of the abdomen and pelvis was performed (Fig. 2), demonstrating a high-grade mechanical bowel obstruction with transition point in the mid abdomen adjacent to a mesenteric soft tissue mass, most likely in keeping with recurrence of the mesenteric B-cell lymphoma. There was interloop free fluid, mesenteric congestion and gas locules adjacent to the soft tissue mass—thought to represent mesenteric venous gas and bowel ischemia.
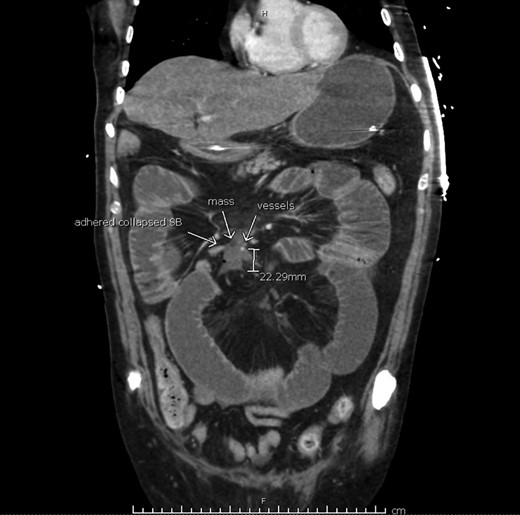
Computerized tomography suggesting tumor recurrence and small bowel obstruction.
The patient underwent a diagnostic laparotomy. Intraoperatively, there was a thick fibrous band originating from an epiploic appendage of the transverse colon to a mass at the root of the small bowel mesentery, causing a closed-loop small bowel obstruction at the level of the mid ileum. Upon further dissection, this mass was found to be the Surgicel® used at the site of the previous mesenteric lymph node excisional biopsy. Complete adhesiolysis was performed without the need for bowel resection.
The patient’s post-operative course was complicated by sepsis requiring inotropic support, acute renal failure requiring hemofiltration and ischemic hepatitis causing coagulopathy. The patient required 5 days of intensive care with a total acute inpatient stay of 27 days before being transferred to subacute care for rehabilitation. He has been subsequently discharged home for further hematology follow-up.
DISCUSSION
Surgicel® is a commonly used hemostatic agent. This case report highlighted multiple issues with its use. Firstly, the presence of Surgicel® on CT was misinterpreted as recurrence of lymphoma. This had the potential to severely alter the patient’s management goals had he not proceeded to the operating theater where it was established that there was no soft tissue mass and it was in fact foreign material. This is similar to cases reported by Buckley et al. and Sandhu et al. [2, 3], where Surgicel® placed on tumor beds appeared to mimic tumor recurrence on imaging, creating a diagnostic dilemma for surgeons. Secondly, Surgicel®, an absorbable hemostatic agent with pro-inflammatory effects, was the most likely cause of this adhesive small bowel obstruction. The authors suggest removal of Surgicel® once hemostasis has been achieved to avoid the above-mentioned potential complications, particularly in patients with suspected or known malignancy.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}