





Abstract
A 47-year-old male who previously underwent emergency surgery for type A aortic dissection presented to the emergency department 4 years later with acute chest pain radiating to his back and a significant drop in hemoglobin. Clinical presentation was concerning for aortic graft failure, but imaging revealed a large (6.0 × 3.2 × 12.8 cm3) soft tissue mediastinal mass that was not present 4 years before. Pathologic analysis revealed a rare thymic cyst with a hemorrhagic component. This was a challenging case from diagnostic and operative perspectives, involving the expertise of both cardiac and thoracic surgical teams.
INTRODUCTION
Fewer than 3% of anterior mediastinal masses are thymic cysts [1]. Congenital cysts are usually discovered incidentally in the first 2 decades of life and are typically small (<6 cm), unilocular, thin-walled lesions without evidence of inflammation. Acquired cysts result from an inflammatory process and occur more commonly in adult men. These tend to be larger and multilocular with variable wall thickness. Acquired thymic cysts may occur after radiation therapy or surgery, or in association with neoplasms such as seminoma or thymic carcinoma [1]. Thymic cysts are usually benign lesions, but malignant transformation is possible [2].
CASE REPORT
A 47-year-old male presented to the emergency department at a primary care hospital complaining of sudden onset, severe chest pain radiating to his back. Four years prior, the patient suffered a type A aortic dissection and underwent emergency surgery that included Dacron graft replacement of the ascending aorta and a mechanical aortic valve. The patient was anticoagulated with warfarin for his mechanical valve. INR 2 days before presentation was 4.3; the patient was advised to reduce his warfarin dose by one half. Vital signs at the outside hospital were reported as temperature 37.1°C, heart rate 86 bpm, blood pressure 141/89 mmHg and oxygen saturation 98% breathing ambient air. The patient appeared comfortable. Cardiopulmonary examination was benign and consistent with a normal mechanical aortic valve. The remainder of the physical exam was unremarkable. Electrocardiogram showed normal sinus rhythm. Complete blood count, electrolytes and renal function were within normal limits; however, hemoglobin was 40 points lower than 2 days before. Troponin was negative. INR was 3.0.
Workup at the outside hospital included computed tomography (CT) of the chest with administration of contrast material. This revealed a heterogeneous collection in the right prevascular space immediately anterior to the ascending aorta measuring 6.0 × 3.2 × 12.8 cm3, concerning for aortic rupture with contained hematoma (Fig. 1, top left and right). Vitamin K 10 mg IV was administered, and the patient was urgently transferred to our tertiary care hospital.
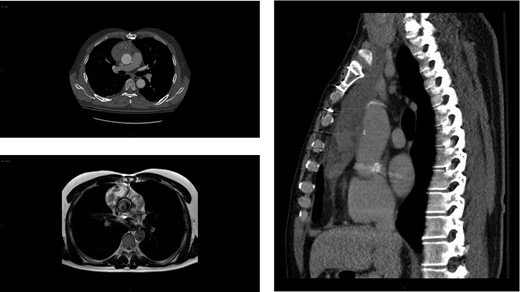
Imaging showing anterior mediastinal mass 4 years after a type A aortic dissection. Axial (top left) and sagittal (right) chest CT images of the large (6.0 × 3.2 × 12.8 cm3) heterogeneous collection in the right prevascular space anterior to the ascending aorta initially concerning for a rupture but contained hematoma. MRI depicting the same heterogenous soft tissue mass (bottom left). Of note, no mass was detected on the chest CT scan performed 4 years prior (not shown).
Upon arrival, the patient was hemodynamically stable with no signs of acute hemorrhage or cardiovascular compromise. The patient was admitted for monitoring and further evaluation. Contrast-enhanced CT scan of the chest was repeated at our hospital. The aortic graft appeared intact with no evidence of contrast extravasation. The configuration of the mediastinal process was stable compared to the outside study 6 h earlier. Furthermore, the appearance of the ascending graft was unchanged from a postoperative study 4 years prior. The anterior mediastinal process was consistent with a lobulated soft tissue mass such as lymphoma, thymoma or teratoma. No additional lymphadenopathy was identified. Review of remote CT imaging performed at the time of the aortic dissection did not demonstrate a mediastinal mass.
The patient underwent evaluation for an undifferentiated anterior mediastinal mass, which included CT abdomen and pelvis, testicular ultrasound and tumor markers. These were negative. Two CT-guided biopsies of the soft tissue mass were non-diagnostic. Cardiac MRI was unable to conclusively characterize the lesion (Fig. 1, bottom left). Given that this mass in the anterior mediastinum defied diagnosis by imaging and biopsy, a decision was made to operate.
Operative planning involved concerns that this may indeed have been a malignant lesion with hemorrhagic transformation or a complication related to the aortic graft, such as infected hematoma or chronic inflammation (Fig. 2). The patient underwent complete resection of the anterior mediastinal mass, which included intubation with a double-lumen endotracheal tube and re-do sternotomy with cardiopulmonary bypass on standby. Intraoperatively, the mass was found to overly and densely adhere to the aorta (Fig. 3, left and middle). There appeared to be an intact capsule with no obvious invasion of adjacent structures. Under lung isolation, the mass was resected in its entirely. All thymic tissue was removed from the upper thymic poles superiorly to the right and left phrenic nerves medially and the diaphragm inferiorly. The mass was adherent to the proximal suture line of the Dacron graft to aorta and required careful dissection to ensure the aorta and tumor capsule were not entered. Frozen section tissue analysis from this anastomotic area was consistent with inflammatory adhesions only. Other analyses of frozen sections at the time of operation were pathologically inconclusive. Given the suspicion of malignancy, the mass was resected with adequate margins for an effective cancer operation if indeed the final histopathological analysis was malignant. Final pathology revealed a large multilocular thymic cyst with evidence of cyst rupture, hemorrhage and organizing hematoma but no evidence of malignancy (Fig. 3, right).
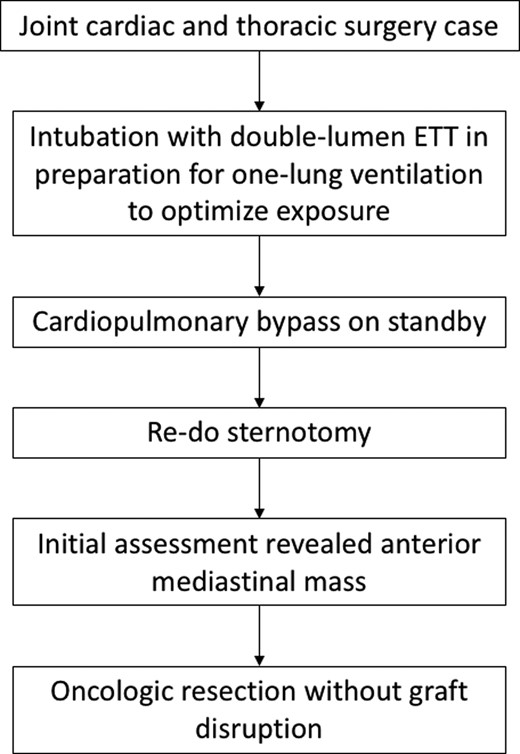
Operative approach.
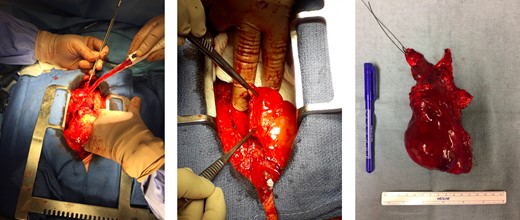
Intraoperative images showing location of lesion and final resected specimen. Intraoperatively, the mass was found to be overlying but densely adherent to the aorta (left). The mass was completely resected with an intact capsule; lesion in situ (middle) and resected specimen (right).
The patient’s postoperative course was uncomplicated. He was bridged with therapeutic dalteparin to warfarin therapy for his mechanical aortic valve. Follow-up in 6 months will include a chest CT scan to monitor for recurrence of the mediastinal mass.
DISCUSSION
This case presents a diagnostically and surgically challenging anterior mediastinal mass. Multilocular thymic cysts are postulated to result from acquired inflammatory processes [3]. We suspect the cyst arose in the inflammatory milieu of the patient’s previous aortic graft. A large thymic cyst developed during a relatively short time interval and was exacerbated by hemorrhage possibly related to anticoagulation for a mechanical heart valve. Although thymic cysts are usually benign, this does not eliminate the possibility of malignancy and therefore surveillance is required [2]. A collaborative approach involving both the cardiac and thoracic surgical teams at our institution optimized the operative management of this rare thymic lesion.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}