





Abstract
Meckel's diverticulum is the commonest congenital abnormality of the gastrointestinal tract. Most cases are asymptomatic and only incidentally found. Its perforation by a foreign body is an extremely rare event. A 53-year-old female presented to Emergency Department with abdominal pain on the right iliac fossa and vomiting. CT scan was performed and showed an intestinal perforation by a foreign body. Diagnostic laparoscopy identified a perforation of a Meckel's diverticulum by a fish bone and a laparoscopic stapled diverticulectomy was performed. Meckel's diverticulum complications are more common in childhood, usually as bleeding. In adults, intestinal obstruction and inflammation are the usual manifestations. Although most swallowed foreign bodies are harmless, in a small number of cases perforation may occur. Preoperative diagnosis of complicated Meckel´s diverticulum is challenging and can often mimic other more common conditions. Laparoscopy is a valuable tool for the diagnosis and treatment of complicated Meckel’s diverticulum.
INTRODUCTION
Meckel’s diverticulum is the most common congenital malformation of the gastrointestinal tract, described in 0,14–4,5% of cadaver dissections [1]. Originally described by Fabricius Hidanus in 1598, the name derives from Johann Friedrich Meckel who illustrated its embryological origin in 1809 [2]. It results from the incomplete obliteration of the omphalomesenteric canal, which typically occurs between the 6th and 10th gestational weeks [3].
Most cases remain asymptomatic and are diagnosed incidentally during imaging studies or surgery [4]. Complications occur in ~4% of the population and may represent a life threatening condition, requiring emergent treatment [1]. The perforation of a Meckel’s diverticulum by a swallowed foreign body is an extremely rare event.
The authors present a case of a perforation of a Meckel’s diverticulum by an intact fish bone.
CASE REPORT
A 53-year-old female patient with dyslipidemia was admitted to the Emergency Department with abdominal pain on the right iliac fossa and vomiting for 24 h. On arrival she was afebrile and haemodynamically stable. Abdominal examination disclosed increased abdominal tenderness with rebound located on right iliac fossa.
Blood tests revealed leukocytosis (14.500 white blood cells/μL) with neutrophilia (79%) and no C-reactive protein elevation; kidney and liver functions both were within normal range. Abdominal ultrasound showed some free fluid in the pelvis and a computed tomography scan was then performed and revealed a linear hyperdense foreign body located in distal ileum with intraperitoneal free air (Fig. 1). A presumed diagnosis of intestinal perforation was established, and patient was taken to the operating theatre for diagnostic laparoscopy.

CT scan evidencing a foreign body in distal ileum with intraperitoneal free air.
Intraoperatively the diagnosis of a perforated Meckel’s diverticulum by a fish bone with localized peritonitis was made (Fig. 2) and a laparoscopic stapled diverticulectomy was performed, with the stapler applied to the base of the diverticulum, transversely to the longitudinal axis of the bowel (Figs 3 and 4).
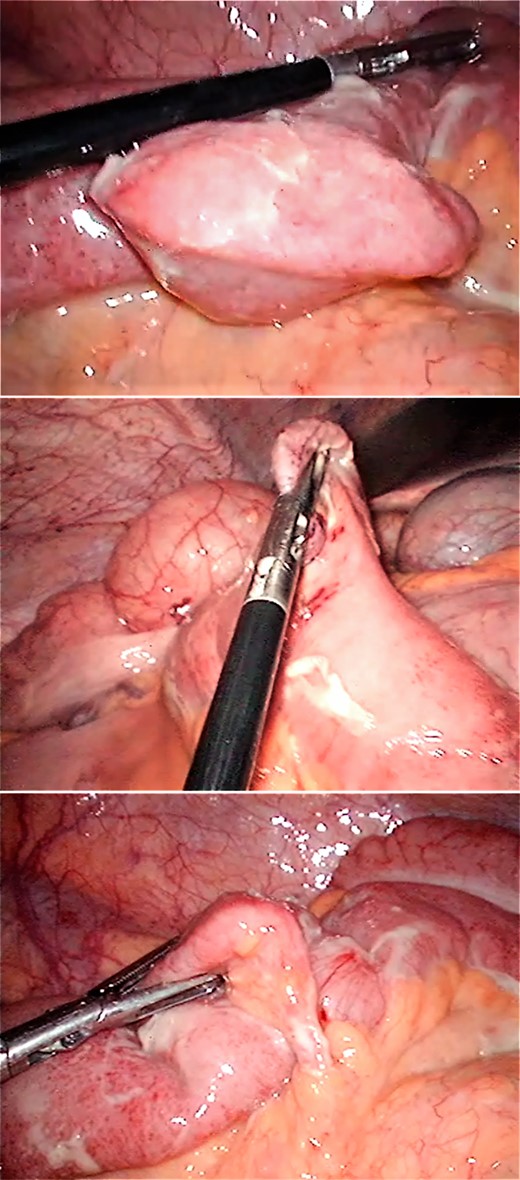
Perforated Meckel´s diverticulum by a foreign body in-situ (fish bone).
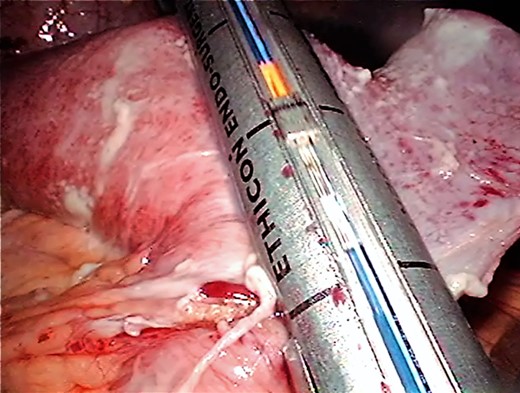
Stapled diverticulectomy.
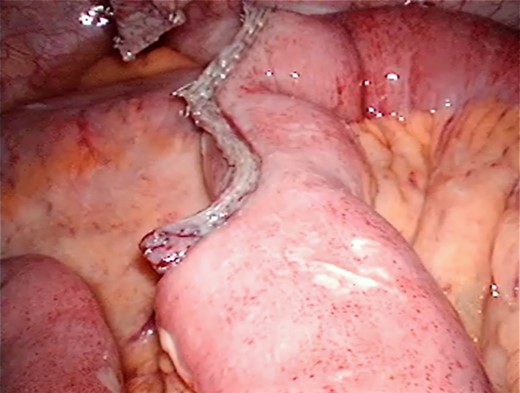
Staple line after resection.
Postoperative course was uneventful, and patient was discharged 4 days after surgery.
Histologic examination of the surgical specimen was consistent with perforated Meckel´s diverticulum, with no evidence of ectopic mucosa.
DISCUSSION
Meckel´s diverticulum is a vestigial remnant of the omphalomesenteric duct, usually located within 100 cm from ileocaecal valve, on antimesenteric border, with an average length of 3 cm [1, 5]. It is a true diverticulum containing all layers of the intestinal wall and its own blood supply from the superior mesenteric artery, which makes it vulnerable to obstruction and infection [3]. Approximately 60% of Meckel’s diverticula have heterotopic mucosa, of which more than 60% are of gastric origin [5].
Complications have higher incidence in childhood, usually as gastrointestinal bleeding. Intestinal obstruction and inflammation that can mimic acute appendicitis are the most common complications in adults [6].
Perforation causes of a Meckel diverticulum include diverticulitis, ulceration of adjacent ileal mucosa due to acid produced by ectopic gastric mucosa and swallowed foreign body. Although most swallowed foreign bodies pass through the gastrointestinal tract without problem, in a small number of cases perforation may occur. In a review of 52 complicated Meckel´s diverticula, 8% underwent surgery due to a perforation by a swallowed foreign body [7]. Reported causes of perforation by foreign body include wood splinter, bay leaf, mellon seeds, chicken bone and fish bone [8].
Preoperative diagnosis is hard as symptoms and imaging features are non-specific. Ultrasound and abdominal computed tomography are usually of little value as it is difficult to differentiate between bowel loops and the Meckel´s diverticulum. Most cases are diagnosed intraoperatively, as in the present case, often mistaken for other disorders [3].
Complicated Meckel's diverticulum requires surgery. Whenever there is a macroscopic involvement of the base of the diverticulum or in case of tumour, a segmental bowel resection with primary anastomosis is recommended. In other cases, simple diverticulectomy with transverse suture, to prevent stenosis, seems acceptable [5].
Several studies report both the safety and the therapeutic value of laparoscopy, in case of complicated Meckel’s diverticula, providing all advantages of minimally invasive surgery like reduced morbidity, early discharge and better cosmesis. Tangential excision of the diverticula with a stapler is adequate, provided the base is normal [9].
In the present case, since the Meckel’s diverticulum base was narrow and intact, a laparoscopic diverticulectomy was performed.
Operative mortality and morbidity for complicated Meckel´s diverticula were 1,5 and 12%, respectively, in an epidemiological study at the Mayo Clinic; the cumulative incidence of late postoperative complications during a 20 years follow-up was 7% [10].
In conclusion, the perforation of a Meckel´s diverticulum by a fish bone is exceptionally rare. Laparoscopy is a valuable tool allowing an earlier diagnosis and a prompt treatment of complicated Meckel´s diverticulum with the advantages of minimally invasive surgery.
Conflict of Interest statement
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}