





Abstract
Fibrous dysplasia is a rare congenital disorder, with abnormal hypertrophy of affected bone. A 17-year-old girl with a protrusion on her right forehead presented and was diagnosed as craniofacial fibrous dysplasia. Although she had no gait problem, her right leg was longer than the other. She had vascular malformation on the right leg. The condition was diagnosed as Klippel–Trénaunay syndrome, which also is a rare disorder. As the prevalence of these disorders is scarce, the probability of coincidental association of them is extremely low. No previous report about the association of fibrous dysplasia and Klippel–Trénaunay syndrome could be found. We concluded that, those two rare congenital disorders arose coincidentally in this patient.
INTRODUCTION
Fibrous dysplasia is a rare bony disorder. It is characterized by benign fibro-osseous proliferation. Klippel–Trenaunay syndrome is also a rare congenital disorder. It is characterized by non-tumorous hypertrophy of hard and soft tissue with venous or lymphatic malformations. Incidence of both disorders is very low. Here presented a young lady with both conditions.
CASE REPORT
A 17-year-old girl referred to us with a chief complain of a painless bump on her right forehead. She also had a projection on the parietal area. She and her family told that the protrusions had been observed since she was below teenage and had not changed for these 3 years. She had no visual impairment. She felt healthy and self-reported no other abnormality. X-ray computer tomography scan showed osseous hypertrophic lesions in frontal and parietal bone (Figs 1 and 2). Ground glass appearance of diploe implied fibrous dysplasia. Frontal sinus was dilated without mucosal hypertrophy or frontonasal duct stenosis. Multiple intra-cranial calcification was observed. She presented no psychomotor disorder.
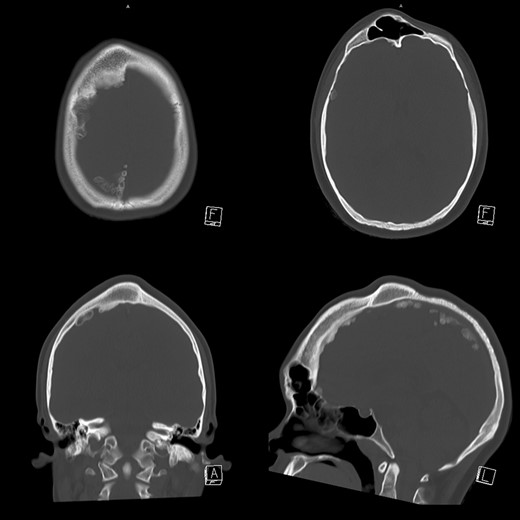
Slices of skull CT. Hypertrophy of right frontal and parietal bone is observed. Diploe of the hypertrophic part presented ground glass appearance. Frontal sinus was dilated without mucous hypertrophy. Intra-cranial calcification was also observed.
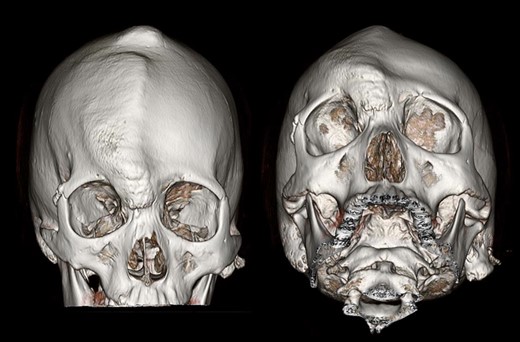
Three-dimensional CT of the patient’s skull. Protrusion of right frontal and parietal area was well observed.
To rule out polyostotic type fibrous dysplasia, further questioning was done. Although she had not realized by herself, physical examination revealed that her right leg was longer than the other (Fig. 3a). Difference in circumferences was not obvious. Subcutaneous venous dilatation on the lateral side of her right leg was observed (Fig. 3b). Standing radiograph of the lower extremities showed leg length discrepancy of 31 mm (Fig. 4). In MRI venography (Fig. 5), vein with large caliber running from right lateral lower leg to great saphenous vein was observed. Venous density in the right leg was higher than the other, suggesting existence of venous malformation. The condition was diagnosed as Klippel–Trenaunay syndrome.
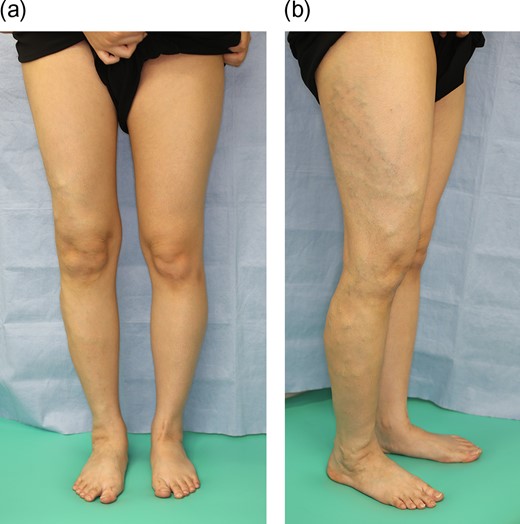
(a) Right knee is at higher than left. (b) Subdermal hyper-vascularity was observed on the lateral part of her right leg.

Standing radiograph of the lower extremities. Leg length discrepancy was 31 mm. Tibial length discrepancy was 21 mm.
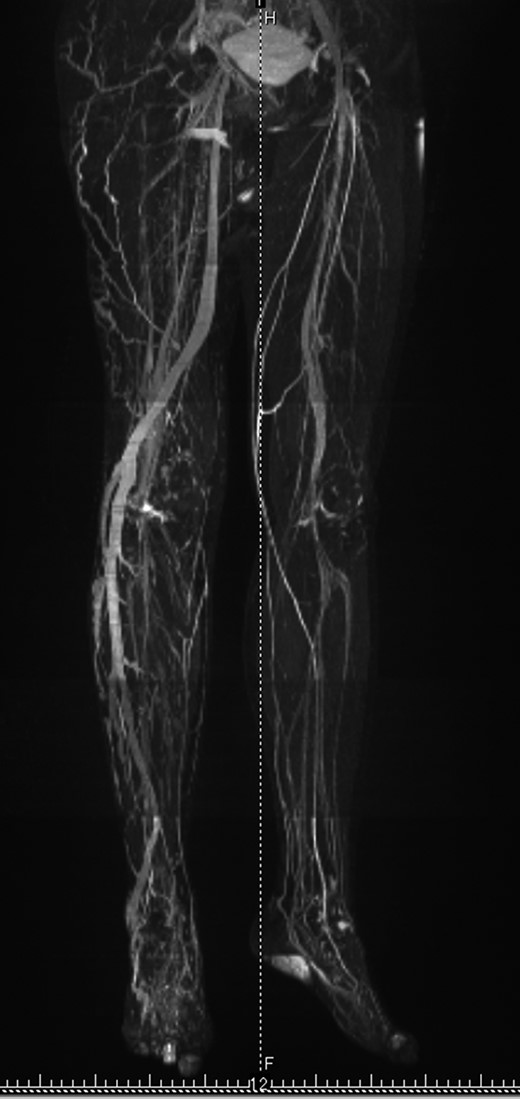
MRI venography of the lower extremities. Vascular density in the right leg is higher than in the left. Abnormally large calibered vessel runs from lateral part of the right lower leg to great saphenous vein.
She sometimes had menstrual cycle abnormalities. She presented microcytic anemia with 7.5 g/dl of hemoglobin. Endocrine tests revealed border line low level of cortisol and adrenocorticotropic hormone. Luteinizing hormone, follicle stimulating hormone, prolactin, thyroid stimulating hormone, growth hormone, somatomedins, renin, aldosterone, dehydroepiandrosterone sulfate and blood sugar test were all within normal range. Café au lait spot was not eminent. No other fibrous dysplasia lesion, other than in skull was found. Thus, McCune–Albright syndrome was denied. Iron was administered for anemia.
Discussion with the patient and her guardians were done for several times. At that time, development of the skull protrusion seemed to be stopped. Reduction of the prominence, not complete resection of the lesions, was planned. No treatment was planned for Klippel–Trenaunay syndrome.
From CT scan images, 3D bony models were printed (Fig. 6). At the time of operation, anemic condition improved (11.0 g/dl of hemoglobin). After coronal incision, scalp flap was raised beneath periosteum, to preserve supra-orbital vascularity of the periosteal, which was to be used in case of frontal sinus cranialization (Fig. 7). With aid of navigation system (StelthStation: Medtronic, Mineapolis, USA), protruded parietal part was shaved with chisels and a motor-driven bur. Most of the protruded frontal bone was shaved in the same way, but lesions near the frontal sinus was scraped with an ultra-sound surgery machine (VarioSurg: NSK-Nakanishi, Kanuma, Japan) to preserve mucosa. Anterior wall of the frontal sinus was removed, but the posterior wall was left intact. Outer table of left intact area was taken and placed as anterior wall of frontal sinus. It was fixed with an absorbable plate and screws (Fig. 8). Donor site of the bone was filled with calcium phosphate cement (Cerapaste: NGK, Komaki, Japan). Total blood loss was 310 ml and no transfusion was done.

3D models made from CT data. Sliced models were also made to observe inner structure. They were referred during the surgery.

The scalp flap was raised subperiosteally. The picture is oriented the orbits and the nose downward. Protrusions on the cranium were observed.
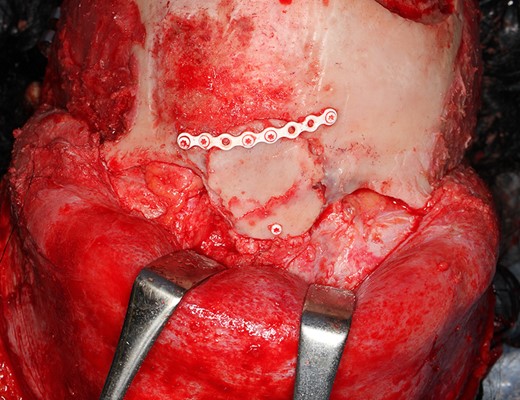
After reduction of the protrusions, anterior wall of frontal sinus was scraped leaving mucosa intact. Outer table of parietal bone was transplanted and fixed with an absorbable plate and screws.
The patient and her guardians are happy with the result.
DISCUSSION
Fibrous dysplasia is a rare condition, that is characterized by benign fibro-osseous proliferation of bone. It was first reported in 1872 [1]. It constitutes 7% of bone tumors [2]. The precise prevalence of fibrous dysplasia is unknown, as many patients are asymptomatic. According to Fibrous Dysplasia Foundation, the frequency is estimated to be one out of every 15 000–30 000 people [3]. Fibrous dysplasia is a genetic disease, in which vertical transmission from parent to offspring is not well-documented. Hypothesis that fibrous dysplasia is the result of somatic mutations that occur at some early stage of embryonic development is generally accepted [4–6] demonstrate that fibrous dysplasia is a disease of the bone marrow stromal cells. The cells, beginning to differentiate osteogenically, altered to proliferate and produce fibro-osseous masses of fibrous dysplasia [4]. The alteration is caused by mutations in the GNAS gene, codes for the alpha subunit of the signaling G protein, Gsα [6].
Klippel–Trenaunay syndrome is also a rare congenital condition, that affects vascular development with hypertrophy of soft and hard tissue. It was originally reported by Klippel and Trenaunay [7]. Hypertrophy of the affected tissue is not neoplastic. The precise prevalence of this syndrome is also hard to presume, but according to Forbes et al. [8], the frequency is estimated to be 2–5 out of every 100 000 births. Somatic PIK3CA mutations are identified in lymphatic malformations associated with Klippel–Trenaunay syndrome [9].
Probability of coincidental association of these two rare disorders is extremely low. Though, at this moment, there was no previous report of the combination of fibrous dysplasia and Klippel–Trenaunay syndrome. Fibrous dysplasia presents tumorous development, but Klippel–Trenaunay syndrome does not. There could not find certainty, offering logical explanation of the association. We concluded that, in this particular patient, those two rare congenital conditions arose by coincidence.
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts of interest relevant to this article to disclose.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}