





Abstract
Metastatic tumors of the appendix is a rare entity, whereas only limited data involving metastasis arising from gastric cancer has been reported. Herein, the case of gastric adenocarcinoma metastasis presenting as acute appendicitis is reported. A 53-year-old male, with a history of subtotal gastrectomy due to gastric adenocarcinoma 3 years before, was referred to the Emergency Department with symptoms of acute appendicitis. While this condition was confirmed intraoperatively, histology examination and comparison with the previously excised gastric specimen indicated that metastasis of gastric adenocarcinoma to the appendix was present. Metastatic appendiceal carcinoma arising from the stomach is an extremely rare condition, associated with poor prognosis. Aggressive treatment of the solitary lesion may present favorable results.
INTRODUCTION
Gastric cancer is a common tumor of high rate of recurrence, that often metastasizes to the peritoneum through lymphatic dissemination or invasion of adjacent structures [1]. Gastric metastasis to the appendix has been rarely described in the literature, being an uncommon cause of acute appendicitis. It is, however, important to be aware of such rare entities that can be encountered intraoperatively, especially in oncologic patients.
Herein, we present the case of a patient presenting with symptoms of right lower quadrant pain and intraoperative findings of gangrenous appendicitis, whose pathologic examination indicated an appendiceal metastasis of gastric adenocarcinoma, operated 3 years before. Further treatment choices are also discussed.
CASE REPORT
The patient, a 53-year-old Caucasian male, presented to the Emergency Department complaining of right lower quadrant pain that initiated 5 days before and for which he followed conservative treatment with antibiotics. During clinical examination, Mc Burney’s sign was present, as well as rebound tenderness on palpation. He did not mention any concurrent symptoms, such as bowel dysfunction, nausea, anorexia or vomiting. While he did not complain about fever during the previous days, temperature on examination was 38.3°C.
His surgical history included gastric adenocarcinoma that was treated 3 years before through subtotal gastrectomy and subsequent chemotherapy; follow-up imaging examinations did not reveal any signs of recurrence. No other health conditions were diagnosed and he was not under any medication. Laboratory blood examination showed elevation of white blood cells (12,75/μL) with 73.5% neutrophils, and CRP levels were 5.82. Imaging examination through chest and abdominal X-ray did not reveal any pathologic findings.
Due to his persistent condition and characteristic findings of examination, the patient was admitted to our Surgical Department and underwent an open appendectomy through Mc Burney incision; intraoperatively, gangrenous appendicitis was confirmed, without signs of perforation and with a small amount of peritoneal fluid (Figs 1 and 2). The postoperative period was uneventful, the white blood count was normalized (6,11/μL with 50.2% neutrophils) and he was discharged in good health condition on the fifth postoperative day.
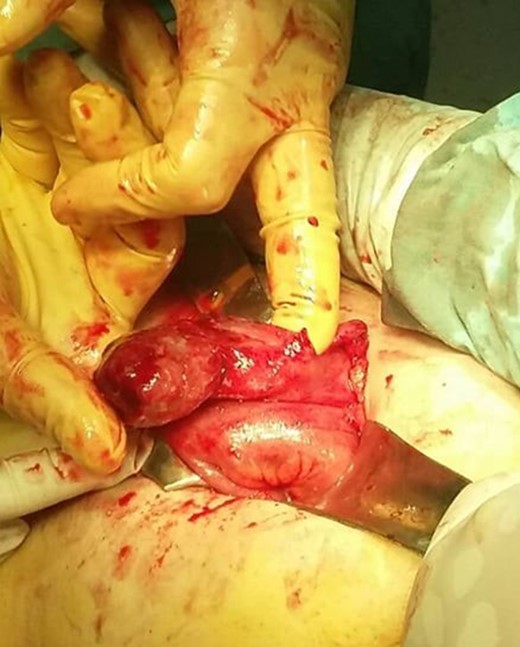
Intraoperative finding of gangrenous appendicitis.

Gangrenous appendix. Excised specimen.
Pathologic examination of the excised specimen revealed extensive metastatic infiltration in all the length of the appendix by highly differentiated adenocarcinoma, leading to extensive mucosal ulceration; surgical margins were disease-free. Comparison with the histologic assessment of the gastric specimen that was excised 3 years ago confirmed the metastatic origin of the appendiceal tumor. More specifically, on immunohistochemistry, positive for epithelial markers CK20 and MNF116, but negative for neuroendocrine markers chromogranin, synaptophysin and NSE, supporting the gastric origin of the metastasis.
The patient was advised to undergo a new abdominal CT scan for disease staging, which showed no further evidence of abdominal metastases or abnormalities, and no further treatment was considered necessary. Regular follow-up examination was scheduled, which did now reveal signs of recurrence after 4 months, when this report was made.
DISCUSSION
Metastatic tumor of the appendix is an uncommon entity, with the primary site usually being in the gastrointestinal and urogenital tract, breast, lung and gallbladder. Gastric cancer metastasizing to the appendix was first described in 1951 by Goldfarb et al., and only a limited number of reports on this condition has been since reported [1–6]. The mechanism of metastasis remains unclear, but it has been hypothesized that the appendix is infiltrated through peritoneal dissemination, or even represent a solitary peritoneal lesion [1].
Appendiceal metastasis can remain asymptomatic and be diagnosed incidentally [2]. However, in most reported cases, as metastatic cancer cells attach to the serosa and later infiltrate all the appendiceal wall layers, lumen occlusion may occur, which results to inflammation, symptoms of acute appendicitis, and even perforation [3].
Differential diagnosis of the metastasis includes primary adenocarcinoma and carcinoid tumor of the appendix [4]. In our case, the lesion did not show immunohistologic characteristics of a neuroendocrine tumor during pathologic examination. As high suspicion of gastric metastasis, due to adenocarcinoma features, was risen, both specimens, the gastric one from the previous operation and the appendiceal one were compared in order to verify the primary tumor.
Patients that present metastases to the appendix arising from a gastric primary tumor are thought to have a poor prognosis. It is considered, though, that, in case of patients that present only a solitary metastasis to the appendix, this finding does not represent an end-stage condition, and therefore could be managed more aggressively [4].
Patients with metastatic tumors of the appendix are considered to present a poor prognosis, but, due to their limited number, further treatment with chemotherapy has been not proved to increase the survival rate. In two cases, the patients followed further chemotherapy treatment; the first died 1 year later [2], and the second one died on the second day of chemotherapy due to tumor lysis syndrome [3]. In other cases no further treatment was decided [1, 4]; however, good results from follow-up examinations were obtained, even 14 months postoperatively [1].
Even though excision of a secondary lesion seems to improve survival, it is proposed that appendectomy does not improve survival when metastatic appendiceal tumor is present [7]. In our case, we decided to treat the excised metastasis as a solitary lesion, which was removed within healthy margins. Intraoperative examination of the peritoneal cavity excluded any other signs of abnormalities of the lower right abdomen; further imaging was also negative for other lesions. No further operation or chemotherapy were considered necessary, as appendectomy removed the lesion and chemotherapy still shows vague results.
CONFLICT OF INTEREST STATEMENT
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial or non-financial interest in the subject matter or materials discussed in this article.

{kind=link}
{kind=link}