





Abstract
The presence of an incarcerated vermiform appendix within a femoral hernia defect, a De Garengeot hernia, is distinctly different than an inguinal hernia containing the appendix, an Amyand hernia. The De Garengeot hernia is a rare finding with few reported cases. We present a 35-year-old female with a painful groin mass palpable below the inguinal ligament. An ultrasound of the groin revealed a thin-walled fluid collection medial to the femoral vessels. No additional imaging at the time was obtained. Intra-operatively, the patient was found to have her distal appendix incarcerated within the transected hernia sac thus altering the planned surgical procedure. We present a unique operative approach for managing a De Garengeot hernia.
INTRODUCTION
Femoral hernias are a rare type of hernia, making up fewer than 5% of groin hernias. A De Garengeot hernia is a rare type of hernia that is defined as a femoral hernia containing the ‘vermiform appendix’. It is an even rarer diagnosis with fewer than 100 cases reported in the literature. The incidence varies between 0.5 and 5% of all femoral hernias [1]. We present a case of an intra-operatively diagnosed De Garengeot hernia in a 35-year-old female and a novel surgical approach used to repair the defect.
CASE REPORT
Our patient is a 35-year-old female who presented with a painful, tender right groin lump for a 6-week duration. An ultrasound revealed a thin-walled fluid collection medial to the femoral vessels (Fig. 1). She was diagnosed with a femoral hernia and offered a repair of the hernia. Due to an improvement in symptoms since onset and clinic visit and in anticipation of the upcoming summer, she opted for elective repair. Unfortunately, her symptoms worsened prior to her surgery date resulting in an expedited operation. The patient was taken to the operating room for repair of her hernia. An incision was made overlying her groin bulge. She was found to have an obvious hernia sac below the inguinal ligament which was dissected from the femoral vessels and pubic tubercle. Due to the small size of the defect, <1 cm, the sac and contents were unable to be reduced into the abdomen. The decision was made to ligate the sac at the level of the defect. After ligation and upon examination, the distal tip of the appendix was found to be within the hernia sac and transected. The decision was made to extend the skin incision laterally in anticipation of accessing the peritoneal cavity. The external oblique, internal oblique and transversalis layers were incised in the direction of their respective fibers. The cecum was identified and brought out of the incision. A window was made at the base of the appendix which was ligated and the completion appendectomy performed. The mesoappendix was then separately ligated. The cecum was returned to the abdomen and the three muscle layers were closed individually. Due to a small amount of spillage, the decision was made to perform a primary repair of the femoral defect. Prolene suture was used to perform the herniorrhaphy, approximating the inferior portion of the inguinal ligament to cooper’s ligament inferiorly. The patient tolerated the procedure well and was discharged to home the same day. The final pathology confirmed acute appendicitis. The patient reported mild abdominal bloating at her 2-week postoperative visit that resolved by her 4-week postoperative visit.
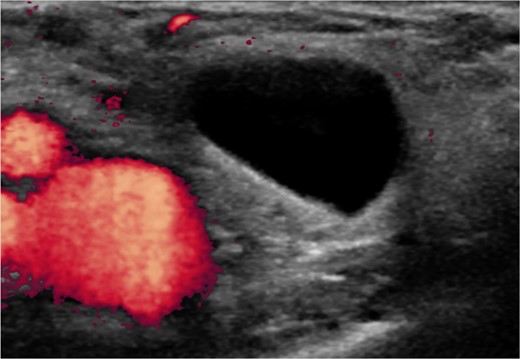
A thin-walled fluid filled sac medial to the femoral vessels diagnostic of a femoral hernia.
DISCUSSION
The De Garengeot hernia is an extremely rare variant of femoral hernias. There are several theories attempting to explain the predisposition to developing a De Garengeot hernia. One suggests that patients have a large or overriding cecum within the pelvis that pushes the appendix into the femoral ring. The next suggests a variable anatomic rotation of bowel during fetal development. Finally, having a relatively mobile cecum may predispose one’s appendix to migration into the femoral canal [2].
Due to the rarity of the pathology, there is no clear standard surgical approach. Some cases describe open approaches with or without mesh and laparoscopic approaches with or without mesh. The decision on approach often is predicated on the pre-operative knowledge of the pathology or its intra-operative identification.
Klipfel et al. performed an emergent right inguinotomy on a 67-year-old female with an incarcerated femoral hernia. The vermiform appendix was found incarcerated within the hernia with signs of necrosis. A conventional appendectomy was not possible due to the length of the appendix and the cecum being inaccessible through the inguinal incision. A laparoscopic appendectomy was performed and the femoral hernia was repaired with a biological mesh using the Rives technique. It was reported the patient recovered quickly and was discharged 2 days later. At 1 month follow-up there were no signs of complications or recurrence [3].
Sinraj et al. describe a 38-year-old female who presented with right inguinal swelling lasting 15 years with pain and vomiting for 2 days. She was found to have an incarcerated femoral hernia. During repair via an inguinal approach, an inflamed appendix was discovered within the hernia. An appendectomy was performed and the femoral ring was closed with polypropylene mesh. Postoperatively, the patient developed a superficial surgical site infection and was treated with intravenous antibiotics [4].
Shiihara et al. describe a two-way surgical approach to treat a De Garengeot hernia. A 74-year-old female was found to have a 3 cm × 3 cm mass below the right inguinal ligament. CT revealed a swelling and an enhanced appendix within the femoral hernia leading to the diagnosis of a De Garengeot hernia. First, the hernia was reduced laparoscopically and a subsequent laparoscopic appendectomy was performed. A hernioplasty was performed using a mesh plug via an anterior approach to prevent preperitoneal contamination. The incarcerated hernia sac was reduced and then ligated and resected laparoscopically. The pathology report revealed acute purulent appendicitis. The postoperative course was uneventful. The patient was discharged on postoperative Day 8 [5].
Unlike other cases reported in the literature, our patient was found to have an incidental De Garengeot hernia discovered intra-operatively, thus altering our planned surgical approach. We performed an open completion appendectomy through the same inguinal incision used to perform the herniorrhaphy. The abdominal cavity was entered and the cecum easily identified allowing the appendectomy to be performed. This approach proved to be safe for the patient while still allowing the procedure to be performed in an outpatient manner without significant postoperative complications or short-term recurrence.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}