





Abstract
Parasitic leiomyomas (PL) are rare intra-abdominal tumors usually found in young women and are considered a type of uterine leiomyomas. They are usually reported in women who underwent laparoscopic morcellation of fibroids and frequently present with symptoms such as abdominal pain and distention. Treatment usually involves en bloc removal of the mass after dividing its blood supply from the host organ. In this case report, we describe the case of a middle-aged female who developed high-grade small bowel obstruction due to compression from a large PL with blood supply from the greater omentum. The patient underwent operative resection of the PL and subsequently fared very well. Meticulous attention to blood supply and attachments of PL to host organs is necessary for safe resection.
INTRODUCTION
Parasitic leiomyomas (PL) are rare intra-abdominal tumors usually found in women of reproductive age group. They are usually reported in women who underwent laparoscopic morcellation of fibroids and frequently present with symptoms such as abdominal pain and distention [1, 2]. We present the case of a PL presenting as a high-grade small bowel obstruction (SBO) in a young female with no prior surgeries.
CASE REPORT
A 45-year-old female presented to our emergency department with a 3-day history of diffuse abdominal pain and obstipation accompanied by bouts of vomiting. She reported increasing abdominal girth over past several years. Her past medical history was significant for fibroids for which she never sought any treatment.
On examination, she appeared mildly distressed but with normal vital signs. Her abdomen was distended and tender to palpation in the right lower quadrant. Her hemoglobin (Hb) was 12.9 gm/dl, white blood cell count was 16 × 103/µl and platelet was 403 × 103/µl. A CT abdomen/pelvis with contrast showed a large intra-abdominal mass with resultant mechanical compression leading to a high-grade SBO (Fig. 1). Several distended loops of small bowel were noted to have thickened walls with surrounding edema raising concern for bowel ischemia.

CT abdomen/pelvis showing large intra-abdominal mass causing high-grade small bowel obstruction.
The patient was taken emergently to the operating room for an exploratory laparotomy. On entering the abdomen, ~500 ml of ascites were suctioned out. A large mass measuring 12 × 12 × 8 cm3 was found with its blood supply arising from the greater omentum and a small fibrotic attachment to the dome of the uterus.
This mass was resected by first dividing its attachment to the uterus using bowie electrocautery. The mass was subsequently eviscerated to expose the vascular pedicle from the omental attachment (Fig. 2). The omental pedicle with its blood supply was ligated and divided en bloc (Fig. 3). The patient was extubated in the operating room and transferred to her room in stable condition. Over the next 5 days, she advanced to a house diet, reported bowel movements, flatus and minimal abdominal pain. On postoperative Day 6, she was discharged home.
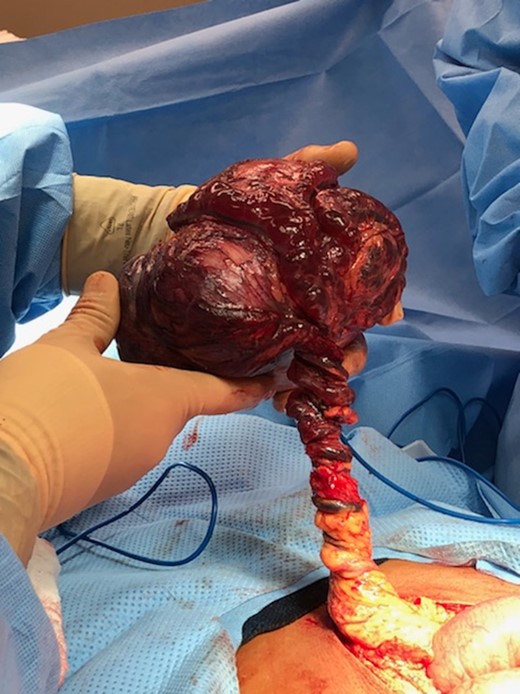
Parasitic leiomyoma with its blood supply arising from the greater omentum.

Resected parasitic leiomyoma along with its vascular pedicle.
On immunohistochemical studies of the specimen, it was found to display lesional cells which were positive for desmin and smooth muscle actin. The tissue was also negative for CD34, S100, CD117, CAM5.2 and HM B45. These findings are characteristic of a leiomyoma. The specimen also exhibited the presence of staghorn vessels but subsequently tested negative for fumarate hydratase deficiency. It did not show any features of hypercellularity, bizarre nuclei, rhabdoid inclusions, alveolar type edema or neutrophilic nuclei with perinuclear halos. After complete pathological examination, the specimen was determined to be a parasitic leiomyoma with secondary infarction.
DISCUSSION
Uterine leiomyoma (UL) is the most common pelvic tumor arising in women [2]. Risk factors primarily include African-American race, nulliparity, obesity, family history and hypertension [3]. International Federation of Gynecology and Obstetrics (FIGO) classify UL into four main types: subserosal, transmural, intramural and submucosal [1]. PL is widely regarded as a subtype of subserosal UL [4].
Historically, PL was thought to arise as subserosal projections from the uterus that latched onto other organs for their blood supply [5]. However, with the introduction of laparoscopic morcellation for fibroids, they are now hypothesized to arise as a result of accidental seeding during morcellation of uterine fibroids for removal during surgery [6]. Our patient did not have any history of prior surgery likely pointing to the spontaneous origin of her PL. It also had a fibrotic stalk attaching it to the uterus, further pointing to the fact that her PL developed as a subserosal projection of her uterus latching on to the greater omentum for its blood supply.
Our patient presented with signs and symptoms consistent with SBO with concern for bowel viability on CT scan. Though not every patient presents with such extreme symptoms, the majority of patients still present with symptoms caused by mass effect [2, 6]. Van Der Meulen, in his systematic review of 69 women with post morcellation PL, noted that most women presented with symptoms, such as abdominal or pelvic pain, dyspareunia, abdominal distension, urinary frequency and constipation. A small percentage of the women (21.7%) were also asymptomatic with PL being an incidental finding [6].
Treatment of PL is usually surgical resection performed open or laparoscopically [7]. Since our patient presented with a clinical picture of SBO with concern for bowel viability, she was taken to the OR emergently for exploration. Intraoperatively, it is also of great importance that time be taken to assess the pathologic blood supply of the lesion. Their blood supply can arise from peritoneum, greater omentum, small or large bowel [5–7] and care must be taken to avoid injury to these other organs inadvertently. Jacobs et al. demonstrated a case of distal ileum obstruction due to uterine leiomyoma in a 64-year-old woman. The patient, post-mortem, was found to have an intraluminal, calcified speculated mass identified to be a uterine leiomyoma which was postulated to have eroded into the ileal wall and detached from its original pedicle via intestinal digestion [8]. One should also be aware of any attachments to the uterus given a variant of PL in patients without prior surgery.
Surgeons also should be aware of other clinical entities that mimic PL. Presence of multiple PL should raise the suspicion of leiomyomatosis peritonealis disseminata [6]. In summary, PL is a rare subtype of UL which can present in symptoms ranging from mild abdominal pain to high-grade SBO. Meticulous examination of the mass’ parasitic blood supply is crucial to safe resection and good outcomes for patients.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}