





Abstract
Small bowel obstruction (SBO) is one of the most common acute surgical conditions that needs immediate innervation to prevent the morbidity and mortality associated with it. The common causes of SBO are different in developed and developing nations. Well-versed knowledge of the rare causes of SBO including its option of management is necessary. In this article, we present a case of an acute SBO secondary to Appendico-ileal knotting. The diagnostic difficulty and the options of management are discussed
INTRODUCTION
Small bowel obstruction (SBO) is one of the common acute abdomen with different causes. Management of SBO needs through knowledge of the pathophysiology and causes of obstruction. The commonest causes include Adhesive SBO, Hernia, volvulus and malignancies [1–3] appendix as a cause of mechanical SBO has been well known since 1901 [4]. this has been described in literatures with different names; appendico-ilial knotting, appendicular tourniquet, appendicular knot and appendiceal tie syndrome [4–7]. It is difficult to make the diagnosis preoperatively as the patients present as SBO. The subsequent management is dictated by the intra operative finding.
CASE REPORT
A 46-year-old-female patient presented with crampy abdominal pain of a week duration. Associated with vomiting of ingested matter which latter become bilious matter. She does not pass faeces but passes flatus. She has abdominal distention for last 4 months which increased since the onset of cramp. On physical examination, she was tachycardia to the level of 110 beats per minute, BP 110/70 and she was maintaining her saturation on atmospheric oxygen-97%. Her temperature 37.2°C, her abdomen was distended with hyperactive bowel sound, hyper tympanic to percussion and no tenderness. On digital rectal examination, normal anal tone with empty rectum and no blood on examining finger. On investigation, she has WBC count of 10 600 with neutrophil 86%, She was referred from private setup with abdominal ultrasound which shows significant dilation of bowel loops with increased peristaltic activity and right lower quadrant blind ending tubular structure with diameter of 18 mm with hypoechoic content. On plain abdominal X-ray shows dilated small bowel loops with multiple air fluid level. (Fig. 1)

Erect abdominal X-ray showing multiple air fluid level with dilated small bowel loops.
With the diagnosis SBO secondary to adhesion band, the patient was taken to the operation room after and the finding was dilated small bowel loops with closed loop obstruction at distal 8 cm of ilium by appendicular knot. At the tip of the appendix there is 4×2 cm cystic mass with no solid component. Retrograde appendectomy including mesoappenix done (Fig. 2). The biopsy result is mucions cyst adenoma with no extension in the surrounding mesoapppendix and the base of the appendix. (Fig. 3) There was a pressure mark exactly at the ileocecal junction and 8 cm away from it. Post-operatively, the patient started sips on second day discharged on fifth day with post-operative diagnosis of SBO secondary to appendico-ilial knotting with appendicular mucocele.
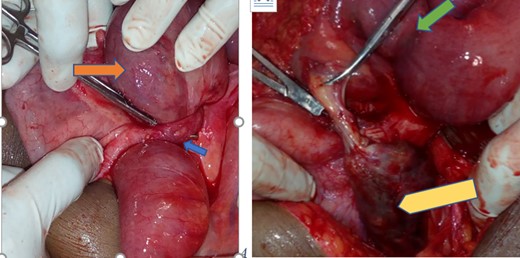
Appendix with mucocele entangling distal ilium forming closed loop obstruction (blue arrow—appendicular knot, orange—entangled distal ilium, green—the pressure mark on the distal ilium and yellow—gangrenous appendicular mucocele).
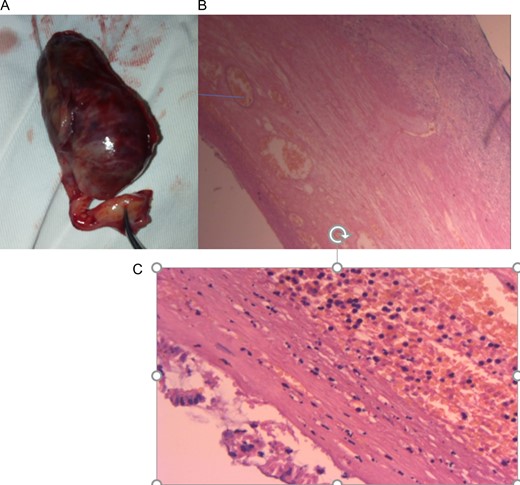
(A) Post-appendectomy gangrenous appendix with mucocele, (B) and (C). Histologic specimen per low power and high power field microscopy showing appendicular mucocele with some haemorrhagic infracts with thinned out mucosa and no extension beyond the submucosa.
DISCUSSION
Acute SBO is one of the most common surgical clinical problems. It can be classified based on many factors: functional or mechanical, the small bowel (SBO) or large bowel (LBO) obstruction, partial or complete, simple, or complicated [2]. Mechanical SBO has many etiologist, post-op adhesion being top in the developed countries. Soressa et al.’s study [1] in Ethiopia post-op adhesion and groyne hernia are the commonest cause of SBO. Other common etiologist includes post-op adhesion and small bowel malignancies [1, 3].
Appendicitis as a cause of SBO has been known in the literature since 1901 when Lucius Hotchkiss reported three successful surgeries for intestinal obstruction due to appendicitis [4]. Bhandari et al. has reviewed the literature and proposed four categories on the pathology of appendicitis causing obstruction; adynamic, mechanical (without strangulation), strangulation of intestine and intestinal obstruction due to mesenteric ischaemia [8].
Strangulation can be due to the appendix wrapping around the base of a bowel loop, or when inflamed appendix adheres to caecum, small intestine or posterior peritoneum and a part of the bowel herniates through the gap. This is described with appendicular KNOT, appendicular tourniquet, appendiceal tie syndrome and appendico-ilial knotting [6, 7, 9, 10]. in our opinion, appendico-ilial knotting is the preferred name because it describes the pathologies of both appendix and ilium.
Diagnosis of SBO is made based on history and physical examination. The four-cardinal sign and symptoms are colicky abdominal pain, vomiting, absolute constipation, and abdominal distension [6]. As depicted in the table, most of the patients with appendico-ilial knotting presented with abdominal pain, vomiting and constipation [4–10] Chatterjee suggest that a period of acute appendicitis precedes the mechanical obstruction. CT scan of abdomen can suggest the diagnosis preoperatively. But as the patients are having acute abdomen, emergent exploratory laparotomy is indicated and it will confirm the diagnosis.
The management depends on the extent of the strangulation and part of bowel involved. It ranges from appendectomy to right hemicolectomy. In our case, the appendix was gangrenous with viable distal ilium so appendectomy was done. The mucocele associated with our case can be ascribed to chronic retention mucus.
CONCLUSION
Appendico ilial knotting is a rare cause of mechanical SBO. As a surgeon dealing with acute abdomen in day to day practise, knowledge about the diagnosis and management of this rare diagnosis is very helpful.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}