





Abstract
Ileostomy formation is a fundamental component in the surgical management of many gastrointestinal diseases and like all intra-abdominal surgeries, small bowel obstruction is a recognized complication. In this paper we discuss a case of a 44-year-old female who previously had a loop ileostomy for slow bowel transit in the presence of spinal bifida. She presented for subsequent total colectomy because of ongoing pain due to chronic colonic dilation. At surgery, the stoma was not revised and the efferent loop was divided at the peritoneal level of the anterior abdominal wall. Six days postoperatively, the patient developed a small bowel obstruction as a result of the remnant efferent loop within the anterior abdominal wall, forming a cystic mass compressing the ileostomy, requiring surgical intervention. As far as we are aware, this is the first case of small bowel obstruction described due to this unusual etiology.
INTRODUCTION
Ileostomy formation is an integral component in the surgical management of many gastrointestinal diseases mainly colorectal surgery and may be permanent or temporary. Specific complications of an ileostomy may be classified according to the time of onset (early or late) and in relation to the procedure (after construction or takedown) [1]. This case report presents an unusual cause for a small bowel obstruction as a complication of an ileostomy.
CASE REPORT
A 44-year-old female who has already had loop ileostomy for slow bowel transit in the setting of spinal bifida presented 12 years later for a total colectomy because of ongoing pain as a consequence of chronic colonic dilatation. A laparotomy was performed for total colectomy but the stoma, being well situated and with good function, was not revised and the surgeon decided to divide the efferent ileal limb at the peritoneal level of the anterior abdominal wall, leaving the afferent ileal limb to function as an end ileostomy.
The patient recovered well with the stoma functioning well until Day 6, when she developed a small bowel obstruction. CT scan demonstrated cystic structure compressing the ileum loop within the anterior abdominal loop just before the stoma opening (Figs 1 and 2). Digital stomal examination and Foley’s catheter failed to pass through the stoma opening confirming the obstruction being at the abdominal wall. Failure of supportive measures, the patient was taken to theatre for revision of the stoma. Per stoma endoscopy was attempted with a gastroscope and which also failed to traverse the compression. At surgery, a semicircular skin incision was made adjacent to the stoma revealing what remained of the efferent ileal loop transformed into cystic mass abutting the stoma causing tight compression and was tightly adherent to the afferent ileal loop (Fig. 3). This was drained and partially excised with limited mobilization of the stoma. The remnant mucosa adherent to the afferent ileal loop was cauterized. Her recovery was unremarkable and was discharged Day 4 postsurgery. Histopathology of the partially excised cyst wall confirmed small bowel with viable mucosa showing mucosal flattening and complete loss of the villi.
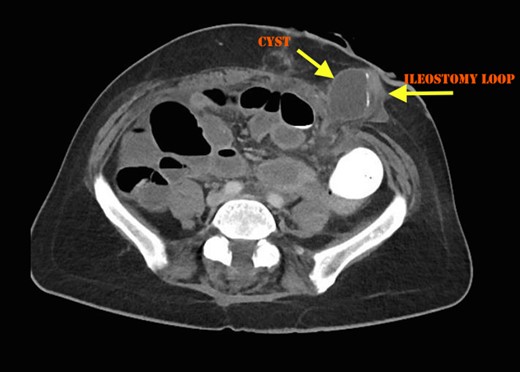
Cross sectional CT Image showing compression of ileostomy opening.
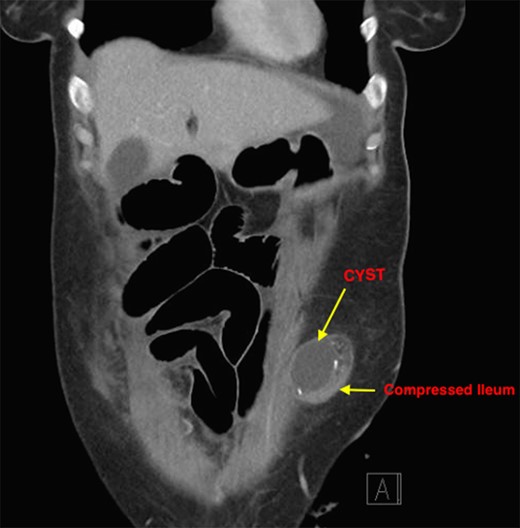
Coronal section showing compression of ileostomy.
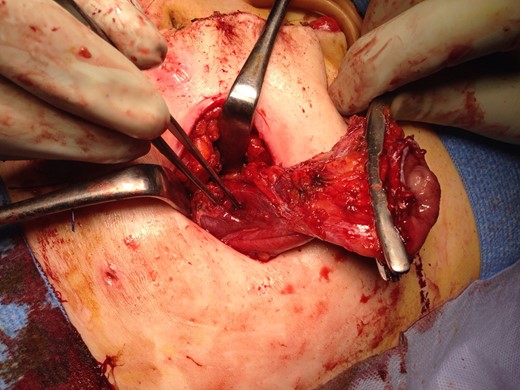
Cystic mass opened confirming remnant of efferent loop.
DISCUSSION
Small bowel obstruction is a recognized complication of ileostomy
Small bowel obstruction may occur because of too small trephine in the anterior abdominal wall, a twisted loop, small bowel adhesions in the area around the ileostomy, intraperitoneal adhesions or an acute parastomal hernia [1].
The incidence of early parastomal herniation and bowel obstruction ranges from 4.6% to 13% [2–5] and usually requires urgent reoperation.
In this unusual cause, the small bowel obstruction, the remnant efferent ileal loop developed into closed loop, because its opening was fibrosed and transformed into a cystic mass, obstructing the afferent loop within the abdominal wall. This option is quite a feasible one to convert a loop ileostomy into a functional end ileostomy, however, one must ensure the efferent loop is patent at its opening. As far as we are aware, this is the first case of small bowel obstruction described due to this unusual etiology.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}