





Abstract
Intestinal duplication is rare congenital pathology generally diagnosed in infancy or early childhood. Presentation in adults is extremely rare. We present a case of a 36-year-old otherwise healthy female patient without any past medical history. She presented with a month of lower abdominal pain, clinical examination revealed pain and a palpable mass in the lower abdomen. CT scan confirmed a cystic mass dependent of the cecum wall and colonoscopy showed an extrinsic compression of the lateral wall of the ascending colon. However, the mucosa and the rest of the colon appeared normal. Since pain became more intense laparoscopy was performed and a cystic mass dependent on the cecum was discovered. Laparoscopic hemicolectomy was performed. Patient underwent full recovery. On follow up controls, pathology described intestinal cystic duplication of the colonic wall.
INTRODUCTION
Duplications of the gastrointestinal tract are congenital anomalies that can occur anywhere in the gastrointestinal tract [1], and are usually diagnosed before the age of 2. Colonic duplications are even rarer comprising only 6.8% of all gastrointestinal duplications [1]. Reports of enteric duplication cysts in adults are extremely rare with only a few cases described, and the majority of them resolved via laparotomy [1, 3].
Gastrointestinal duplications usually share a common wall with the adjacent portion of the bowel, but may or may not have communication with it [1]. The treatment of symptomatic colonic duplications is en bloc resection of the cyst and adjacent viscera. Occasional small cystic duplications can be excised without bowel resection if there is no compromise of blood flow to the intestinal segment [2].
We report a case of a female patient with colonic duplication cyst resolved with laparoscopic approach.
CASE REPORT
Patient is a 36-year-old woman without any past medical history, she was complaining of lower abdominal pain for about a month. Clinical examination revealed a palpable mass in the lower abdomen. A contrast-enhanced abdominal computed tomography (CT) revealed an 8 × 8 × 6 cm3 cystic lobulated mass dependent of the cecum wall, without any lymph nodes of hepatic masses (Fig. 1A). Complete blood count and laboratory exams were normal. Colonoscopy demonstrated an extrinsic compression of the lateral wall of the ascending colon. However, the mucosa and the rest of the colon appeared normal (Fig. 1B).

(A) CT revealing a 7 × 8 cm2 cystic lobulated mass dependent of the cecum wall. (B) Colonoscopy showing extrinsic compression of the lateral wall of the ascending colon. (C) Colonic mass and right colon.
Since the pain continued to persist, surgery was planned and a laparoscopic approach was decided. A 8 × 7 × 6 cm3 cystic mass was discovered that covered and was completely attached to the cecum and ascending colon, no vascular pedicle was identified and no lymph nodes or other masses were found, in light of this, a right laparoscopic hemicolectomy was performed with autosutures (Supplementary Video).
The right colon with the mass was completely resected through a small midline incision without complications. The external surface of the mass was pinkish-gray color and the cystic wall was even in thickness ~0.4 cm (Fig. 1C) and contained clear mucous fluid. Pathology reported intestinal duplication cyst, microscopically, the cystic wall partially consisted of normal mucosa, submucosa, smooth muscle and serosa (Fig. 2A and B). No epithelial dysplasia or malignancy was evident.
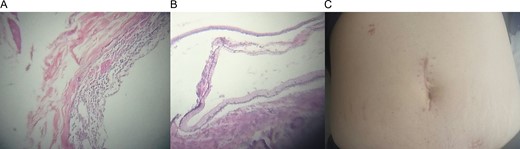
(A) Microscopic view of the cystic wall. (B) Normal colonic wall adjacent to the cystic wall. (C) Midline incision after recovery.
The postoperative course of the patient was uneventful, she initiated soft diet a day after surgery and was discharged once full diet was resumed.
On follow up controls patient was completely asymptomatic, without any pain or complications (Fig. 2C).
DISCUSSION
Duplications of the gastrointestinal tract are rare congenital anomalies [1] since they were first described by Calder in 1733 [5] their incidence of such abnormalities have been low, from 1 in 18.000 [2] to 1 in 4500 [5]. In adults, only a few cases reports have been described and mostly resolved through laparotomy [1, 3, 4].
The pathogenesis of alimentary tract duplications is controversial and many theories have been described [4], but abnormal recanalization after the solid epithelial stage of embryonic bowel development is thought to be the underlying cause [1].
To match the criteria for intestinal duplications, four criteria are needed; a vacant structures that consist of a muscular coat, usually two layers; they should be lined with epithelium that resembles that of the gastrointestinal tract; they usually extend to some portion of the alimentary tube and are tightly attached to it; and the type of epithelial lining at the duplication is not necessarily consistent with that part of the gastrointestinal tract to which it is attached [4].
All of the criteria for intestinal duplication were met in our patient.
The most common clinical manifestations of colonic duplications are a combination of pain and or obstructive symptoms. These symptoms may be the direct effects of distension of the cystic duplication or caused by compression of adjacent organs [1]. Our patient presented with a month of abdominal pain, that became that became increasingly intense, as the mass continued to grow.
Duplications are classified according to their location (ileum 30%, ileocecal valve 30%, duodenum 10%, stomach 8%, jejunum 8%, colon 7%, rectum 5%), shape—cystic (80%) or tubular—and presence of ectopic tissue within the duplication (gastric mucosa) present in up to 50% of the cases [2].
Preoperative diagnosis of colonic duplication is often difficult. Plain abdominal x-ray may reveal a cystic, gas-filled structure. Ultrasonography may also be a useful imaging modality; however, the diagnosis is best established with CT imaging or contrast enema. Contrast studies will demonstrate a filling defect or luminal communication with the bowel if there is in fact one [10]. Complete excision of the duplication is the preferred treatment, except in cases in which extensive involvement is present or vital structures are jeopardized [7], to avoid any future complications, including the possibility of malignant degeneration [6].
For these reasons we attempted to treat the mass with a laparoscopic approach since compared with open right hemicolectomy, laparoscopic right hemicolectomy has the advantages of minimal invasion, faster recovery, and a lower rate of wound infection, and it can achieve the same degree of radicality and prognosis as open right hemicolectomy [9].
Duplications cysts can be a complicated diagnostic in surgical practice because of the low incidence of presentation especially in adults, however, they should always be considered in the differential diagnosis of abdominal cystic lesions [8]. For this, a high index of suspicion is necessary to facilitate prompt and quickly intervention for a complete patient recovery, also in a unique way our patient prove the great variability of surgical options for a single pathology as rare as duplication cyst.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}