





Abstract
A 61-year-old woman presented with chronic anterior pain and stiffness in the distal left thigh. Examination revealed swelling and tenderness immediately proximal to the patella. Radiographs showed opacities in the distal anterior thigh whilst MRI identified enlargement of the distal quadriceps tendon with splayed fibres separated by solid conglomerates. Dystrophic calcification of the quadriceps tendon was diagnosed. Blood tests revealed no systemic abnormalities in calcium handling. Arthroscopy of the left knee identified calcific deposits in the supra-patella pouch with surrounding synovitis. An open debridement of the tendon was performed; biopsy of the excised tendon showed chronic tenosynovitis with dystrophic calcification without evidence of malignancy. Post-operatively her knee was braced in extension enabling progressive flexion over 4 weeks. Anterior knee pain diminished post-operatively and 10 months following surgery the patient was pain free, able to walk normally and scored 99/100 on the Fulkerson modification of the Lysholm score.
INTRODUCTION
Quadriceps tendon calcification is seen on ~10% of knee radiographs [1], however, such lesions almost always immediately adjoin the patella [2] appearing as ‘whiskers’ or ‘flecks’ [3, 4]. The calcification reported in this case report involved the entire quadriceps tendon, is the most extensive reported in the literature and posed a significant therapeutic challenge.
CASE REPORT
A 61-year-old woman presented to a knee surgeon with a 6-month history of pain in the distal anterior left thigh accompanied by ipsilateral knee instability and stiffness. Pain was exacerbated by walking up and down stairs, squatting, kneeling and was worse at night, whereas resting the knee in extension alleviated pain. The patient was otherwise well and without history of previous knee injury. She had power walked 6 miles daily for many years. Salient medical history included shock-wave treatment for left-sided rotator cuff calcification many years previously. On examination, there was tenderness 3–4 cm proximal to the left patella associated with effusion and quadriceps wasting.
Plain radiographs and an MRI scan of the left knee were undertaken.
Radiographic appearance and MRI signal change confirmed calcification rather than ossification or enthesopathy. An unusual diagnosis of dystrophic calcification of the left quadriceps tendon was made (Figs 1–4).

Weight-bearing lateral radiograph of the patient’s knee shows extensive mineralization of the quadriceps tendon.
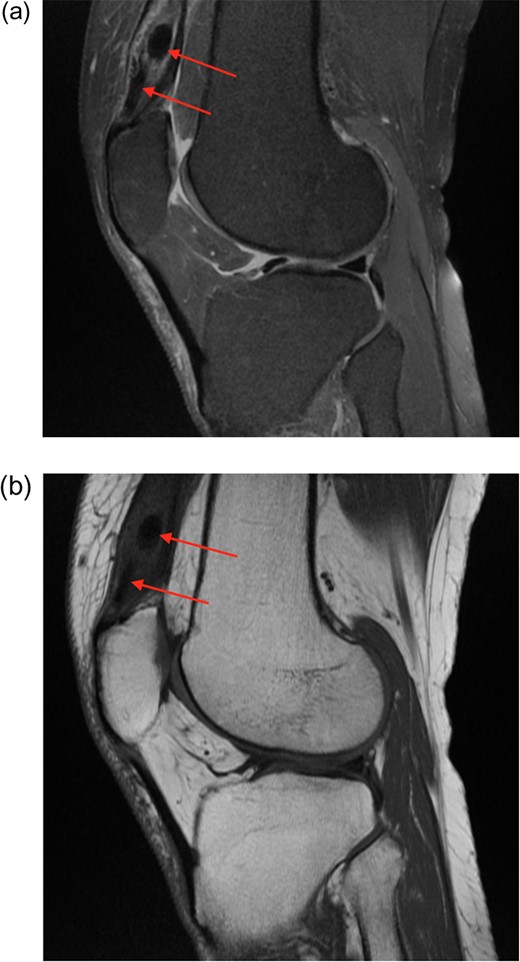
(a) Proton density fat saturated (PDfs) sagittal MRI. There is enlargement of the distal quadriceps tendon, with splayed fibres separated by solid low signal foci. (b) T1 sequence MRI also showing low signal lesions.
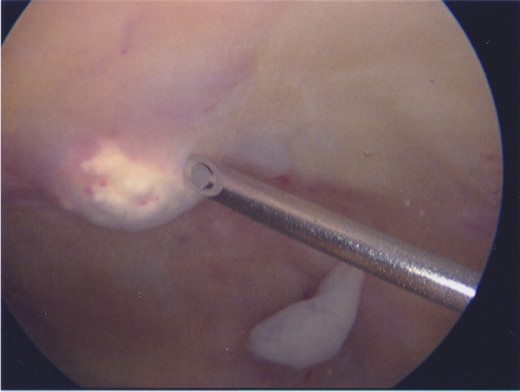
The supra-patellar pouch of the knee during arthroscopy. A focus of calcification is seen protruding into the joint, left of the tip of the needle. Note the erythematous synovitis overlying the calcification. Loose material below the needle shaft is believed to be fibrotic synovium.

The patient’s knees 10 months after surgery. Note the healed incision on the left knee.
Electrolytes and renal function, bone profile, parathyroid hormone, ESR and CRP were unremarkable.
Despite conservative management, her symptoms continued and she was offered surgery.
The surgical procedure began with an arthroscopy. Synovitis was identified in the supra-patella pouch where foci of calcified material protruded from the quadriceps tendon. An arthroscopic shaver was used to excise calcified deposits, prior to open operation.
Using a 12 cm longitudinal incision in the distal anterior thigh, the quadriceps tendon was exposed and ~10% of the tendon was excised to remove as much of the visible calcification and surrounding paste-like material as possible. Calcific foci in the deeper part of the tendon involving vastus intermedius were removed preferentially. The synovial layer was closed, followed by tubularization of the remaining tendon and closure of the wound. The knee was splinted in extension and the patient was discharged from hospital, fully weight-bearing on the left leg, on Day 3 following surgery. Her bracing was diminished gradually, enabling progressive flexion over 4 weeks. Two weeks post-operatively, the patient was more comfortable than prior to surgery.
Histology of the excised material revealed chronically inflamed synovium as well as fibrous tissue with aggregates of calcific material without evidence of dysplasia or malignancy.
Ten months following surgery the patient was pain free and could flex her left knee to 120°. The Fulkerson modification of the Lysholm score was 99/100 [5].
DISCUSSION
Calcification of the entire quadriceps tendon has not, to our knowledge, been previously reported. Calcification has previously been associated with other pathologies, such as chondrocalcinosis [2], uraemia [6] and quadriceps rupture [7, 8] and calcification is believed to be a cell-mediated event [9]. In this case, however, the trigger for calcification was unclear given no evidence of abnormal calcium handling or any history of knee problems. The pathology observed in this case was most likely heterotopic calcification even though no history of injury was noted. It is noteworthy that this patient had been diagnosed with a rotator cuff calcific tendinopathy previously which might have predisposed her to quadriceps calcification.
Arthroscopy confirmed synovitis in the supra-patella pouch in those regions where calcified material was present. This patient’s pain was likely caused by the synovitis overlying the calcific foci, rather than the calcification itself, given the rich sensory innervation of synovium [10].
Given the extensive calcification, the surgical challenge was clear: excision of a significant portion of the quadriceps tendon is incompatible with quadriceps function. If the tendon is detached from the quadriceps muscle it is impossible to insert a substitute tendon given the complexity of the musculotendinous junction. In this case, with the judicious use of linear incisions in the tendon, much of the abnormal tissue was excised. Although the knee became stiff as a consequence, it did progressively loosen. Surgical excision successfully alleviated pain. Nearly 2 years following the operation, the patient is walking without pain or significant restriction.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}