





Abstract
Compound volvulus is an uncommon cause of acute abdomen and involves the twisting of the loops of ileum around the base of the sigmoid or vice versa. It is a surgical emergency that is often missed pre-operatively. We are reporting this case and reviewing the relevant literature to increase the awareness of this condition. A 37-year-old female presented at the Emergency Unit of our hospital with features thought to be acute peritonitis secondary to typhoid perforation and a differential of rupture appendix. She had laparotomy with the finding of a gangrenous twisted terminal ileum around the base of the sigmoid for which a right hemicolectomy and sigmoidopexy were done. Compound volvulus, though rare, can still be encountered in our environment. Prompt identification, adequate resuscitation and expedient intervention will reduce morbidity and mortality.
INTRODUCTION
Compound volvulus, also known as Ileosigmoid knotting or double volvulus, is the twisting of the ileum around the base of the sigmoid or vice versa [1, 2]. It is a rare surgical emergency with very high morbidity and mortality because of its rapid progression to gangrene [1, 3].
Pre-operative diagnosis is often difficult due to non-specific features [1, 2].
This is to report a case of a compound volvulus in a 37-year-old female and review relevant literature in order to increase the awareness of this condition.
CASE REPORT
A 37-year-old female presented at the Emergency Unit with a 3-day history of abdominal pain which was colicky, central initially but later became generalized. It was associated with several episodes of bilious vomiting and abdominal distension. There was a preceding history of diarrhea but had no previous episode of abdominal pain.
On examination, she was in painful distress and dehydrated. Her respiratory rate was 30 cycles/min; Pulse rate was 124 beats/min; blood pressure was unrecordable and temperature of 36.3°C. Abdomen was distended, tender with guarding and rebound tenderness. Bowel sound was absent.
A diagnosis of acute peritonitis secondary to typhoid perforation to r/o ruptured appendix was made. Chest X-ray was normal with no air under the right hemidiaphragm. Plain abdominal X-ray showed dilated loops of bowel and multiple air–fluid levels.
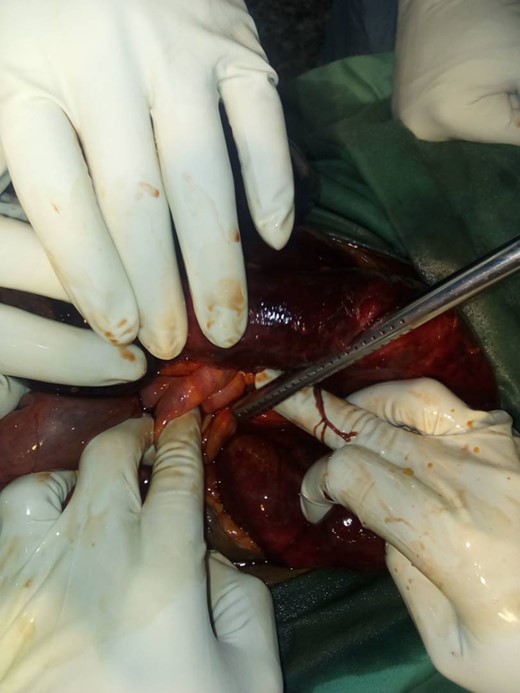
She was resuscitated and had laparotomy. Intra-operative findings were hemorrhagic peritoneal fluid, distended gangrenous 120 cm terminal ileum twisting around distended viable sigmoid colon which had a narrow base (Figs 1–3). She had right hemicolectomy with ileocolic anastomosis and sigmoidopexy. Her post-operative period was uneventful and was seen in the clinic after discharged.

The gangrenous small bowel and the arrow indicates the viable sigmoid.
The knotting point.

The resected small bowel.
DISCUSSION
Compound volvulus is a life-threatening closed loop type of intestinal obstruction. It was first reported by Parker in 1845 [1, 3]. Its incidence is not known. It is more common in Africa, Asia and Middle East than in the Western countries [3] and very few cases have been reported in Nigeria, but none in the North-East [4–7].
Compound volvulus is more common between the third and fifth decades and more in males [1, 2, 4]. Our patient though a female, falls in this age group. The aetiology is not well understood. However, a long mesentery with a narrow base and ingestion of high bulky diet after fasting are the major predisposing factors [2]. Other predisposing factors include lax abdominal wall, post-operative adhesion, intestinal herniation, Meckel’s diverticulum and malrotation [2].
Compound volvulus is classified into [1, 2]:
| Types | Description |
| I | Ileum around the sigmoid |
| II | Sigmoid around the ileum |
| III | Ileocaecal around the sigmoid |
| IV | Undetermined |
| A | Clockwise |
| B | Anticlockwise |
Newer classification which correlates with mortality [1, 2, 8]:
| Class | Description |
| 1 | No risk factor (such as advanced age, co-morbidity), non-gangrenous bowel. |
| 2 | Risk factor, non-gangrenous bowel. |
| 3 | Shock, non-gangrenous bowel. |
| 4 | Gangrene of ileum or sigmoid, no shock. |
| 5 | Gangrene of ileum or sigmoid and shock. |
| 6 | Gangrene of both ileum and sigmoid. |
Our patient had type I, class 5 compound volvulus which was a high risk for mortality.
Clinical presentation is usually of sudden onset of symptoms and abdominal pain is a constant feature [1, 9, 10]. Others include vomiting, abdominal distension, constipation, anorexia and/or diarrhea. There may be hematemesis and rectal bleeding [2]. Fever may be an indicator of gangrene. On examination, patient may be toxic, in painful distress, febrile and/or dehydrated. The abdomen may be distended, tense, tender with signs of peritonitis. Bowel sound may be hypoactive, hyperactive or absent and rectum may be empty.
X-rays are not specific but shows features of intestinal obstruction. CT scan or MRI gives better diagnostic result and useful in making pre-operative diagnosis [1, 10].
Prompt resuscitation is very crucial for survival and includes fluid and electrolytes correction; passage of a nasogastric tube; urinary catheterization for urinary output monitoring and antibiotics. Emergency laparotomy is done as soon as possible. If there is a gangrenous bowel, a single staged procedure of resection and anastomosis may be done or a two-staged procedure of resection and stoma, then stoma reversal at a later date depending on the state of the patient [1, 2]. For non-gangrenous bowel, untwisting of the twisted bowel with or without preventing procedures such as sigmoidopexy, mesopexy, mesoplasty or resection and anastomosis [1, 2].
The prognosis depends on early presentation, diagnosis and prompt intervention. The mortality rate is 6.8–8% for non-gangrenous and 20–100% for gangrenous [2]. Shock is a major cause of death.
CONCLUSION
Compound volvulus, though rare, can still be encountered in our environment and should be considered in cases of intestinal obstruction. It has a very high mortality due to its rapid progression to gangrene. Prompt identification, adequate resuscitation and expedient intervention will improve outcome.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}