





Abstract
Cholecystectomy leads, occasionally, to the diagnosis of subclinical primary carcinomas and rarely metastatic tumors. The authors report the diagnosis of gallbladder metastasis after an elective cholecystectomy for symptomatic cholelithiasis. Histological examination disclosed a metastasis from a lobular breast carcinoma. Authors found no more than 25 case reports of breast cancer metastasis in English literature. Of those, only one reports first diagnosis after elective cholecystectomy with no radiological or macroscopic signs of malignancy. Rare clinical presentations, as in this case, should always be kept in mind specially in high volume centers. These rare presentations lack good quality evidence and challenge the best standard treatment regimen available. Multidisciplinary assessment is the key to maximize the risk/benefit of different treatment modalities. In this case report, although curative surgery was attempted, progression disease was typical of an advance staged disease.
INTRODUCTION
Cholecystectomy is one of the most performed surgical procedures worldwide due mostly to symptomatic cholelithiasis or acute cholecystitis.
Histopathological assessment of surgical specimen is mandatory. Not infrequently, it represents the first evidence of subclinical carcinomas, most commonly of primary biliary origin and rarely incidental metastatic disease.
The authors report breast cancer diagnosis after an elective cholecystectomy for symptomatic cholelithiasis.
CASE REPORT
A 76-year-old woman, with past medical history of breast lumpectomy for a fibroadenoma and an Eastern Cooperative Oncology Group (ECOG) performance status score of 0, was admitted for a routine cholecystectomy due to symptomatic cholelithiasis.
Pre-operative ultrasound examination revealed gallstones and a regular thin gallbladder wall. The patient underwent laparoscopic cholecystectomy. Intra-operative findings were unremarkable. The post-operative period was uneventful and the patient was discharged within 24 h after surgery.
Histopathological examination showed chronic cholecystitis, gallstones and a small subserosal and muscularis foci of isolated small cells with scattered glandular pattern (Fig. 1a). The immunohistochemical evaluation was negative for calretinin and cytokeratin 20 (CK20) and highly positive for cytokeratin 7 (CK7) and estrogen receptor (ER) (Fig. 1b and c). Gallbladder metastasis of breast cancer was diagnosed and the patient was referred to the breast cancer unit at our institution.
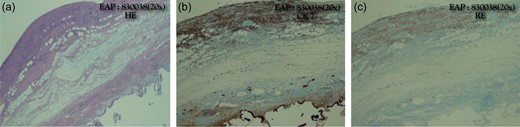
(a) Gallbladder histological analysis: chronic cholecystitis with lithiasis and small subserosal and muscularis foci of isolated small cells with a scattered glandular pattern. (b and c) Immunohistochemical profile showed negativity for calretinine and cytokeratine CK20 (b) and highly positivity for CK7 and estrogen receptor (c).
Physical examination was unremarkable, namely with no signs of breast, axilla lumps or other suspicious findings.
Diagnostic mammogram revealed a 15 mm lump in between the right breast upper quadrants—BIRADS 3. Core needle biopsy was performed, showing a hyalinized fibroadenoma. Thorax, abdomen and pelvis CT scans as well as bone scintigraphy did not reveal metastatic disease. Multidisciplinary team decision was to maintain close surveillance and repeat radiological evaluation in three months. Re-evaluation mammogram and ultrasonography revealed a highly suspicious mass in the upper outer quadrant of the right breast (Fig. 2). No further breast or axillary suspicious radiological abnormalities were detected. Core needle biopsy showed a lobular invasive carcinoma, positive for (CK7) and negative for E-cadherin. No vascular or lymphatic invasion were present. The 100% of cells were positive for estrogen and progesterone receptors, negative for HER2 and Ki67 was 20%. PET/CT scan showed no abnormal hyper metabolic lesions.
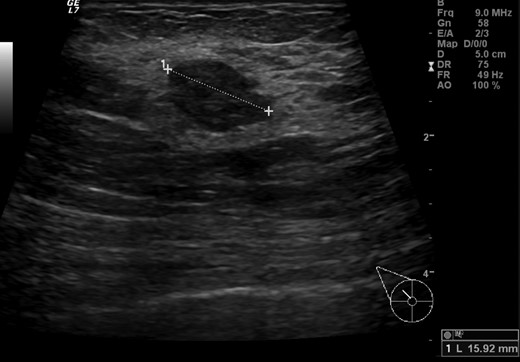
Breast ultrasonography showing an irregular 15 mm hypoechoic lump with no acoustic shadowing between right upper quadrants.
Multidisciplinary assessment, decided to proceed with oncological surgical treatment. Lumpectomy with a negative frozen section sentinel node biopsy was performed. The pathology specimen demonstrated an invasive lobular carcinoma, with lymphatic invasion and lymph node macrometastasis—pT1b G1 N1a(sn) R1 (posterior deep margin)—TNM classification, seventh edition. The 100% of cells expressed estrogen and progesterone receptors. HER2 was negative. Radiotherapy, chemotherapy and hormonal therapy was proposed.
Due to lymph node macrometastasis, and according to the 2013 Breast Cancer NCCN guidelines, complementary elective axillary radical lymph node dissection (Berg level II) was performed. Of the 18 lymph nodes analyzed, 14 were positive for lobular carcinoma (macrometastasis). Post-operative was uneventful. Sixteen months after surgery, bone metastasis was found on scintigraphy performed due to refractory pelvic and lumbar pain. The patient started treatment with everolimus and exemestano. And 36 months after surgery she died due to disease progression.
DISCUSSION
Frequent diseases with typical clinical presentations should always be the first considered diagnosis. However, less frequent or rare etiologies or clinical presentations should always be kept in mind. These challenging cases are even more frequent as highly differentiated and high volume centers emerged. Multidisciplinary assessment with an efficient communication between surgeons, radiologists, pathologist and oncologists is the key factor for a risk/benefit treatment success, since data available regarding these exceptional cases, is lacking.
Brest carcinoma has been considered a systemic disease since its onset. It usually spreads to bone, lungs and to the liver [1]. Metastatic patterns of lobular and ductal carcinoma of the breast are different, with gastrointestinal, gynecological, and peritoneum–retroperitoneum metastasis being more prevalent in lobular carcinoma [2].
Gallbladder is a rare location of metastatic breast cancer. Less than 25 case reports are described in Medline English literature [3–10]. Most of the reported cases, patients were submitted to cholecystectomy with pre-operative ultrasound findings of irregular wall thickening, compatible with acute cholecystitis and a vast majority of them with previous medical history of surgical treatment for breast cancer. Only one case, reports an elective cholecystectomy due to symptomatic cholelithiasis [6].
The interesting nature of this case has to do with the fact that the diagnosis of breast cancer was due to discrete findings in histological assessment after elective cholecystectomy for symptomatic cholelithiasis; and even after histological diagnosis, clinical and radiological evaluation were negative for breast cancer.
In this case report there are two major points to highlight: the rare form of presentation of a high incidence disease; the presentation as a metastatic luminal B invasive lobular carcinoma, which challenges the risk/benefit of potential therapeutic approaches. In the multidisciplinary team assessment, considering the ECOG PS 0, and the fact that no other metastatic sites were found in staging exams, curative surgery was decided, though the patient had metastatic breast cancer at presentation.
Frequently, for rare presentations of common diseases good quality evidence is lacking. Therefore, treatment strategies should be supported by wise clinical judgment and risk/benefit assessment in multidisciplinary teams.
Although curative surgery was attempted after incidental resection of a solitary metastasis, the patient had a typical systemic metastatic disease progression with a discrete survival.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}