





Abstract
Cardiac tumours represent around 0.2% of tumours overall, and primary cardiac tumours are even more uncommon. We report the case of a 72-year-old female with a 7 cm × 4 cm right atrial mass which was prolapsing through the tricuspid valve. The mass was resected and histological analysis confirmed a myxoma. This report describes a rare finding of a giant right atrial mxyoma and subsequent surgical management.
INTRODUCTION
Cardiac tumours are rare findings mainly described in case reports, representing around 0.2% of tumours overall, and primary cardiac tumours are even more uncommon [1]. Myxomata are the most common type of primary cardiac tumour [2]. Most are located in the left atrium but they have very rarely been found in all four chambers of the heart [1].
CASE REPORT
A 72-year-old female presented to her General Practitioner with a brief history of shortness of breath at rest. Her General Practitioner referred to her local hospital for an outpatient transthoracic echocardiogram, which revealed a right atrium of normal size, with a mobile mass prolapsing through the tricuspid valve. This was suspected to be a large thrombus or a mass of unknown origin. In addition, the echocardiogram showed severe aortic stenosis; the aortic valve was trileaflet with rheumatic appearance.
She was transferred to our hospital for potential operative management of the right atrial mass. Repeat echocardiography at our hospital confirmed these findings, showing a large echogenic mass filling the right atrium (5.3 × 2.5 cm2) with severe aortic stenosis (Fig. 1).
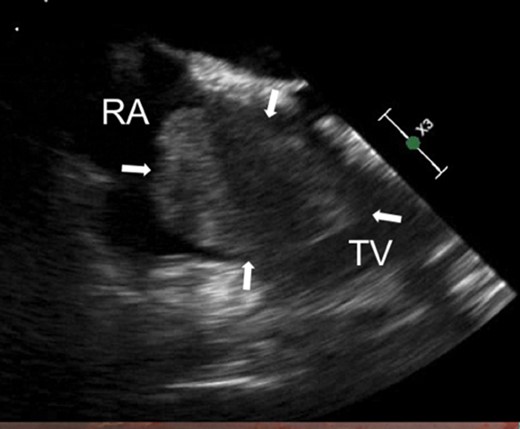
Arrows indicate large right atrial myxoma via transthoracic echocardiography. RA, right atrium; TV, tricuspid valve.
CT cardiac angiogram showed a large filling defect within the right atrium and dense calcification within the aortic valve leaflets (Fig. 2).
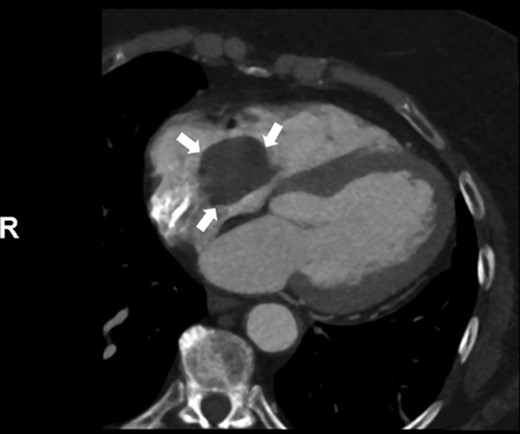
Arrows indicate large right atrial myxoma on CT scan.
Following median sternotomy, the patient was found to have a large right atrial mass measuring 7 × 4 cm2 occupying the majority of the right atrium with a stalk originating at the junction of the superior vena cava and the right atrium. The apex of that large mass was obstructing the outflow of the tricuspid valve. In addition, there was severe aortic stenosis secondary to calcification of the aortic valve. That valve was bicuspid but tricommisural as a result of fusion of the left and right coronary cusps. The patient consequently underwent a right atriotomy of the right atrial mass (Figs 3 and 4). A low transverse aortomy was also performed and a 25 mm TrifectaTM GT prosthesis was sited.
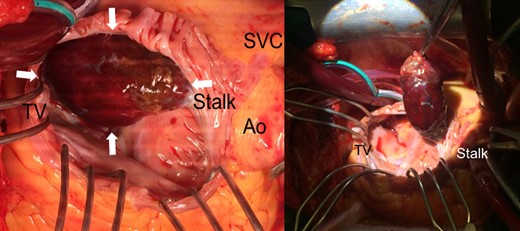
Right atrial mass in situ, looking at the patient from the left. Close up on the left and prior to excision on the right. TV, tricuspid valve; SVC, superior vena cava; Ao, aorta.
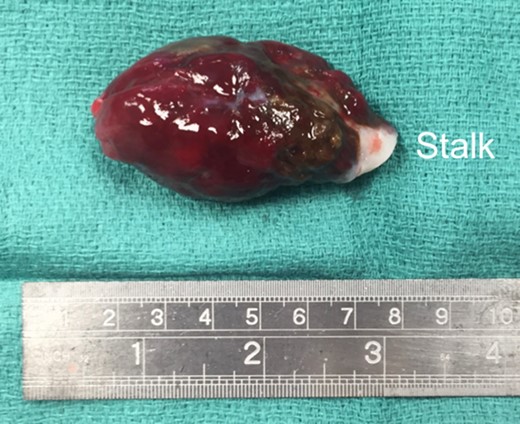
Right atrial mass measuring 7 cm in length.
Histological analysis confirmed the lesion was in keeping with an atrial myxoma with superadded prominent haemorrhage and surface thrombus formation. There was a degree of nuclear pleomorphism in the myxoma cells but no hypercellularity or mitotic activity.
The patient had a slow postoperative recovery but this was anticipated due to a high body mass index and a previous stroke with residual deficit. She was nevertheless discharged 17 days after surgery with routine cardiothoracics follow-up.
DISCUSSION
Clinical presentation is variable but common symptoms and signs reported in cases include dyspnoea, oedema and constitutional symptoms (fever, weight loss) but is dependent on the site, size, mobility and surface [1, 3–6]. Right atrial myxomata can present with obstructive symptoms that imitate tricuspid stenosis and these are also the most common cause of tricuspid valve impedance [3]. Right heart failure and thrombus are appropriate differential diagnoses of a right atrial myxoma. A serious complication of a right atrial myxoma is pulmonary embolism and a chest CT is recommended to rule this out if a patient is symptomatic with breathlessness [7]. The most useful investigations are likely to be transthoracic and or transoesophageal echocardiogram.
Symptomatic myxomata are surgically excised as soon as possible after diagnosis due to the risk of pulmonary embolism and worsening obstructive symptoms [8]. Surgical management provides immediate and continued symptomatic relief, has low peri-operative risk and low mortality: a series of 37 cases (mixed left and right myxoma) reported only one death (2.7%) [9]. A long-term follow-up of 27 patients with surgical excision of right atrial myxomata demonstrated reasonable prognosis and low mortality [10]. The recurrence rate has been reported as 5.4% in left and right myxomata, and serial echocardiography was recommended post-operatively [9]. A report of 12 patients with left atrial myxomata suggested that the total excision of the interatrial septum is strongly associated with no recurrences over 13 years of follow-up [6].
Resection with adequate margins and careful intra-operative handling therefore are essential to prevent recurrence and the risk of further surgical management.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
No funding declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}