





Abstract
Osteochondral fracture (OCF) in the weight-bearing surface of the lateral femoral condyle, associated with patellar dislocation, is an uncommon lesion. We report three cases of acute lateral patellar dislocation with large OCF in the weight-bearing portion of the lateral femoral condyle. In patients with lateral patella dislocation or lateral femoral condyle OCF, careful physical examination, radiography and MRI are recommended to rule out any associated injury.
Introduction
Several authors have described osteochondral injury following patella dislocation. These injuries were to the patella and the lateral trochlear portions of the lateral femoral condyle [1–3].
Osteochondral fracture (OCF) to the weight-bearing surface of the lateral femoral condyle, associated with patellar dislocation, is an uncommon lesion and more posterior than would be expected [4–8].
In this study, we report three cases of acute lateral patellar dislocation with large OCF in the weight-bearing portion of the lateral femoral condyle. In all three cases, OCF was fixed through lateral parapetellar arthrotomy and patella dislocation was treated conservatively.
Case presentation
Case1
A 19-year-old male came with right knee pain and effusion after a non-contact injury of the knee during a football game. The knee had marked effusion with tenderness over the medial border of the patella. Radiography showed large OCF in the weight-bearing area of the lateral femoral condyle [Fig.1Aand B]. CT scan showed bony fragments from the medial border of the patella [Fig. 1C]. Three months after surgery, radiography showed complete healing of the injury with the full knee range of motion (ROM) [Fig. 1D and F].

Case 1. A and B Radiography showing lateral femoral condyle OCF. C, CT scan showing OCF and patellar avulsion fragment.D and E, 3 months postoperative radiography showing complete union.
Case2
A 16-year-old male came with right knee pain and swelling after a twisting injury of the right knee while trying to break a wooden object with his left foot. Radiography showed a large OCF at the weight-bearing portion of the lateral femoral condyle [Fig.2A and B]. CT scan showed the bony avulsion from the medial facet of patella and the lateral femoral condyle OCF [Fig. 2C]. MRI showed lateral subluxation of patella [Fig. 2D]. Radiography, three months after the operation, showed complete union and the knee ROM was full [Fig. 2E and F].
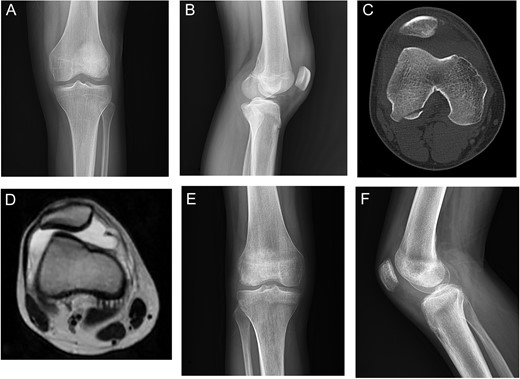
Case 2. A and B Radiography showing lateral femoral condyle OCF and marked effusion. C, CT scan showing lateral patellar subluxation with medial patellar avulsion fracture and lateral femoral condyle OCF. D, MRI showing lateral patellar subluxation and marked joint effusion. E and F, 3 months postoperative radiography showing complete union.
Case3
A 16-year-old female came with a history of falling down and knee twisting at the bathroom. She complained that her knee got deformed and reduced immediately on the field. Radiography showed a displaced OCF in the weight-bearing portion of the lateral femoral condyle [Fig.3A]. CT scan showed displaced femoral OCF and lateral patella subluxation [Fig. 3B]. With lateral parapatellar knee arthrotomy, the femoral OCF was reduced and fixed with bio-absorbable screws [Fig. 3C and D]. Her condition has not been followed up since then.
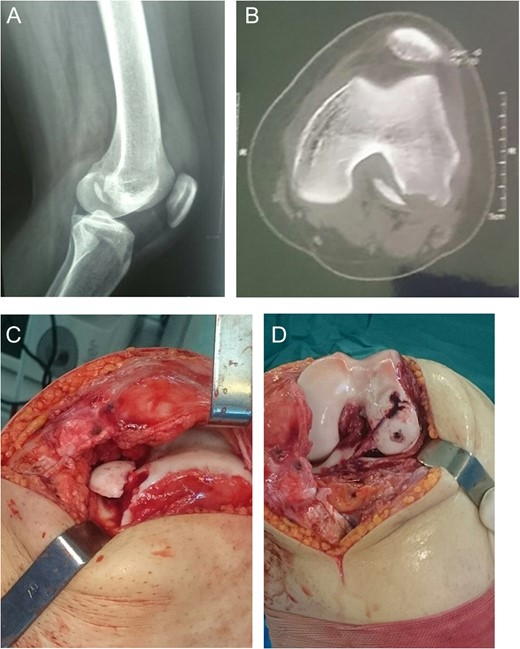
Case 3. A, Radiography showing lateral femoral condyle OCF. B, CT scan showing OCF and lateral patellar subluxation. C and D, Intraoperative photography showing weight-bearing position of OCF and fixation with bioscrews.
Discussion
Lateral patellar dislocation typically occurs with the knee during the early flexion. Vastus lateralis contraction forcefully compresses the patella on the trochlear articular surface.
During dislocation, the patella lies on the trochlear anterolateral margin, producing the typical pattern of injury involving the medial of the patella and the non-weight-bearing portion of the anterolateral femoral condyle [5]. Acute knee pain, with or without trauma and knee effusion, should raise suspicions about patellar dislocation associated with the osteochondral defect [4, 5]. In patients with suspected lateral patellar dislocation, careful palpation of the lateral femoral condyle, especially in flexion, is recommended [2, 3].
Mashoof et al. have described seven cases of patellar dislocation with OCF of the weight-bearing portion of the lateral femoral condyle; it was produced by a non-contact injury. They suggested that these injuries might be the result of a patella dislocation that occurs with the knee in deep flexion. Another suggested mechanism was that shear forces across the mid-lateral femoral condyle from tibiofemoral came in contact in valgus rotation [2]. Similarly, in our study, all injuries were the result of non-contact pivoting injury. Callewier et al. have reported a 23-year-old man with a osteochondral fragment from the weight-bearing portion of the anteroinferior aspect of the lateral condyle, associated with fracture of medial patellar margin consistent with prior lateral patellar dislocation sustained during a martial sport exercise [5].
Nomura et al. have reported 37 osteochondral injuries in 39 patients with acute lateral patellar dislocation. Twelve of them had articular cartilage damage of the lateral femoral condyle [6]. Nomura and Inoue has examined with arthroscopy 30 knees with acute lateral patellar dislocation. Among the 30 knees, 29 had cartilage injury of the patella. There was no cartilage damage on the femoro-trochlear aspect [7]. Beran et al., in their retrospective study of 80 adolescent patients with acute patellar dislocation, have shown that 22 knees in 21 patients had weight-bearing lesion of the lateral femoral condyle. Only in four patients, osteochondral injury was identified on plain radiographs [3]. Nakagawa et al. [8] have described two patients with osteochondral injury of the weight-bearing surface of the lateral femoral condyle associated with lateral dislocation of the patella, suggesting friction between the patella and lateral femoral condyle when the patella was dislocated or reduced at about 90 degree flexion of the knee joint. Because of large fragments, all patients in our study were treated by open reduction and fixation with screws and pins through a lateral arthrotomy. Patella dislocation in all three cases was treated non-operatively with immobilization and muscle strengthening exercises. Chan et al. reported a 12-year-old male with patellar dislocation. Plain radiograph of the knee did not reveal any bone injury. However, knee MRI revealed a large area of chondral delamination in the central weight-bearing portion of the lateral femoral condyle, which was fixed with polylactide fixation nails [9]. MRI examination in acute patella dislocations, especially with effusions and tenderness over the weight-bearing lateral femoral condyle, should be standard, as the incidence of osteochondral injuries is high and cannot be reliably diagnosed using plain X-rays [3, 6, 10].
In patients with lateral patella dislocation or lateral femoral condyle OCF, we recommend careful physical examination, radiographic and MRI imaging to rule out any associated injuries.
Disclosure
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Conflict of Interest Statement
M.J., A.B., H.H. and S.G. declare that they have no conflict of interest.

{kind=link}
{kind=link}
{kind=link}