





Abstract
A Japanese baby was born with a polypoidal projection with hair, on the lateral corner of upper eyelid. The tumour had extent to bulbar sub-conjunctival area. He presented no other malformation nor pathological symptoms. There was no sign of association with Goldenhar, hemifacial macrosomia, epidermal nevus or linear nevus sebaceous syndromes. The tumour was resected at his age of 4 months. The ocular conjunctiva was incised but not excised. Histopathologically, it was mainly consisted of multi-lobuled mature adipose tissue, dense fibrous tissue was observed at the centre of mass, assumed to be the link of palpebral tarsal plate to lateral canthal ligament. As for the location and component, the tumour was diagnosed as a lipomatous hamartoma. Detached tarsal plate was reattached to the lateral canthal ligament. Satisfactory result was achieved aesthetically and functionally. Congenital lipomatous hamartoma, with protuberant appendage appearance on eyelid, without syndromic association, is presented.
INTRODUCTION
Congenital polypoidal mass on eyelid often has association with syndromic diseases. Distinctive condition is that with Goldenhar syndrome [1]. Besides that, organoid nevus syndrome [2] or linear nevus sebaceous syndrome [3] can be reckoned. Here, we present an atypical case with polypoidal mass on the lateral corner of his upper eyelid. The baby showed no other of symptoms, associated with those syndromes.
CASE REPORT
A Japanese boy was referred because of an polypoidal projection on the lateral corner of his left upper eyelid (Fig. 1). The baby was born to a parent, whose family history was unremarkable, after normal gestation and delivery. Hairs were observed on the surface of the projection. Accompanied sub-conjunctival mass was also observed. He had no trouble in opening and closing of his eyes. The baby presented no other malformations or symptoms, including those of Goldenhar, hemifacial macrosomia, epidermal nevus and linear nevus sebaceous syndromes.

A polypoidal appendage was seen on the left lateral corner of upper eyelid. On the surface, hair was observed. Sub-conjunctival extent could be seen.
The appendage was resected when the baby was 4 months old, under general anaesthesia. Continuity of the mass with both palpebral tarsal plate and lateral canthal ligament was confirmed and cut (Fig. 2). Sub-conjunctival dissection was easily done with hydro-injection. The ocular conjunctiva was incised but not resected. The mass was soft and multi-lobuled. It seemed to be consisted of adipose tissue, macroscopically. Incised ocular conjunctiva was sutured with VICRYL RAPIDE™ suture. Detached upper and lower palpebral tarsus was sutured to the lateral canthal ligament with 5-0 VICRYL™ suture (Fig. 3). Aesthetically satisfactory result was achieved. No functional deficit has been recorded so far (Fig. 4).

Upper and lateral margin of the tumour was incised. Continuity to palpebral tarsal plate and the lateral canthal ligament was cut.

Immediately after the operation. Detached tarsal plate was fixed to the lateral canthal ligament.

Two months after the operation. No aesthetic and functional deficit was observed.
Grossly, protruded part of the mass was covered with sparsely haired skin. Sub-conjunctival part was covered with thin capsule with vasculatures (Fig. 5). Histopathologically, most part of the mass was composed of mature adipose tissue, lobuled by fibrous septum with vasculatures (Fig. 6). Outer surface was covered with squamous epidermis with normal rete ridge. In dermal layer, appendages, including hair follicles, sebaceous glands and sweat glands were seen (Fig. 7). Dense fibrous tissue was seen surrounded by the adipose tissue. This was assumed to be the link of palpebral tarsal plate (Fig. 8). No lacrimal grand tissue was identified.

Gross observation of the excised tumour. Vasculature was observed on the surface of lobular sub-conjunctival part.
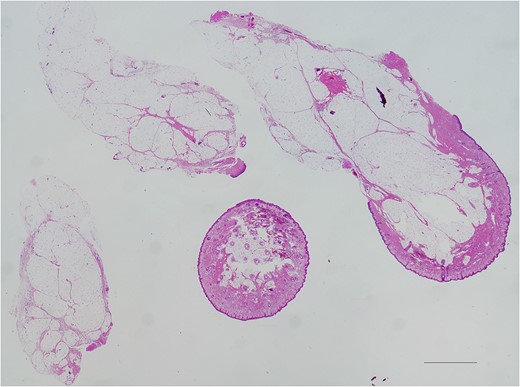
Low magnification observation, taken with ×2 objective lens and stitched. Hematoxylin and Eosin stained. Black bar represents 500 μm. Most part of the tumour was composed of adipose tissue, lobuled by fibrous septum.
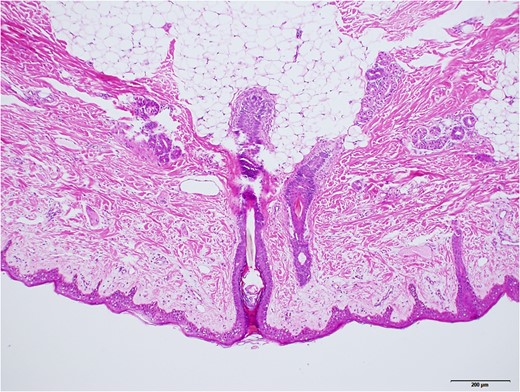
Higher magnified surface area, taken with ×10 objective lens. Black bar represents 200 μm. Mature hair follicles, sebaceous glands, and sweat glands were observed.
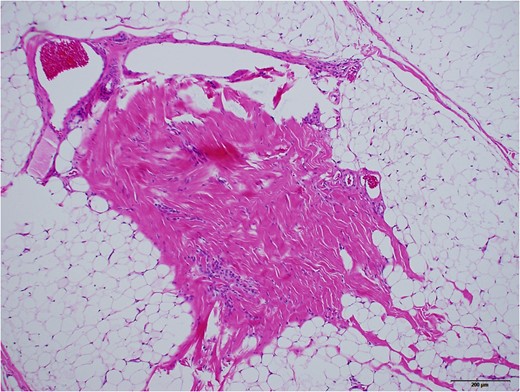
Dense fibrous part with vasculature, surrounded by adipose tissue, assumed to be the link of tarsal plate. ×10 objective lens. Black bar represents 200 μm.
DISCUSSION
It was not easy to classify this tumour as a choristoma [4, 5] or a hamartoma [6]; the former represents normal tissue in abnormal location, and the latter represents normal tissue with abnormal amount in normally given location. Typical dermolipomas seen on the ocular surface, where adipose tissue is rarely seen normally, is classified as a choristoma. Present tumour, mainly composed of adipose tissue, had extent from palpebral region to sub-conjunctiva. Sub-conjunctival part was relatively small. Histologically, in dermolipoma, the delicate collagen of the conjunctival substantia propria is substituted with vascularized thick collagen bundles that resemble those in the reticular dermis of the skin [7]. In our case, sub-conjunctival dissection was not with difficulty. Hence, we surmised the tumour as a lipomatous hamartoma.
Protuberant appendage on lateral canthus is known that it has often related to syndromic diseases, e.g. Goldenhar [1], hemifacial macrosomia [8], epidermal nevus [9] and linear nevus sebaceous syndrome [3]. Though, the baby presented no other external malformation, nor neural disorder.
Caution has been advised to excise a mass locating sub-conjunctival or upper-lateral corner of fornix [10]. Cases of blepharoptosis, keratoconjunctivitis sicca, diplopia, forniceal shrinkage and strabismus have been reported. Preserving conjunctiva on the mass as possible is recommended to prevent symblepharon. In our case, conjunctiva could be preserved, fortunately. Defect of upper eyelid was ~6 mm. Primary closure was able to be achieved without trouble.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}