





Abstract
Eccrine angiokeratomatous hamartoma is a rare newly defined vascular lesion of the skin, the first case of which was reported in 2006 (Kanitakis J, Ly A, Claudy A. Eccrine angiokeratomatous hamartoma: a new variant of eccrine hamartoma with angiokeratoma. J Am Acad Dermatol 2006; 55: S104–6). On web Literature Search, Only three previously documented cases of the lesions were found. A 1.5-year-old female child presented with a painless lesion on her right leg since birth which has been gradually increasing in size and recently developed central ulceration. Histological examination of the excised lesion confirmed the diagnosis. This is the first of the cases to be reported in paediatric age-group (<2 years)
INTRODUCTION
Eccrine angiokeratomatous hamartoma (EAKH) is a newly defined vascular lesion of the skin, the first case of which was described by Kanitakis et al. [1]. It has a unique histology with features derived from two well-established vascular lesions affecting the skin: solitary angiokeratoma (SAK) and eccrine angiomatous hamartoma (EAH). Angiokeratoma is a common condition that presents as a single or many papular lesions on the extremities of young adults [2]. EAH is a relatively rare lesion that is present at birth in ~50% of patients or appears later in childhood in around 25%, while cases of adulthood are also recognized [3]. No. of cases with EAH reported in the literature are very few (<100). Since its recognition, even fewer cases (<5) of EAKH have been documented until now. We present here one such case in a 1.5-year-old female child which is first case report below 2 years of age.
CASE REPORT
A 1.5-year-old girl child presented with multiple painless, flesh-colored lesions (total 3 in number) over the posterior aspect of her right leg since birth. The lesions have gradually progressed in size to attain the present size of 4 × 3 cm2 (largest one) with central ulcers. It was accompanied crusting. Other similar lesions without ulcer of the size 3 × 1 cm2 and 1.5 × 1 cm2 were present superiorly. All the lesions were of irregular shape and had well-defined demarcation from normal skin. No one else among her immediate family had the similar lesion. Doppler report of the lesion ruled out any increased vascularity thus ruling out the suspicion of a haemangioma. FNAC also pointed out towards a hamartomatous lesion and advocated for a detailed examination for confirmation. The lesion was surgically excised and was submitted for histopathological examination (Figs 1–4).

Gross examination of the lesion.

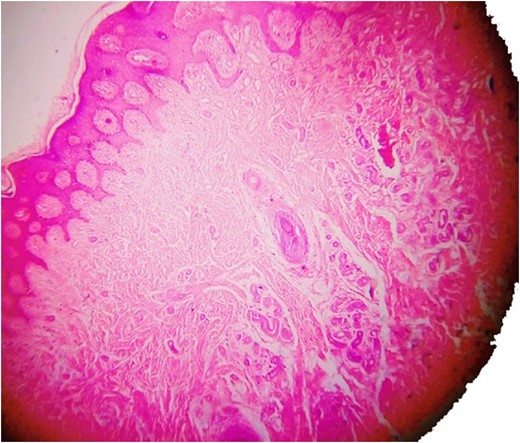
The superficial layer of the lesion showing angiokeratoma (haematoxylin and eosin).
Haematoxylin and eosin staining showing eccrine angiomatous hamartoma.
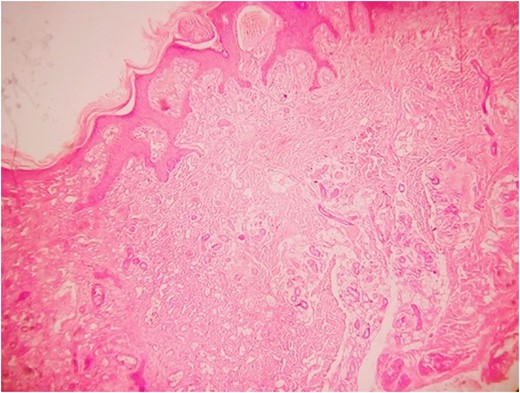
Another magnified section from showing thick walled capillaries.
The superior lesions were closed by primary closure and the lower one was covered by a split skin graft.
Histopathology examination revealed grayish white to grayish brown lesions with hyperkeratitis of the epidermis and focally hyperplastic stratified squamous epithelium. Papillary dermis with numerous dilated, thin walled congested capillaries and the deep dermis with increased number of eccrine glands and numerous capillary channels intermingled with eccrine structure. The stroma was composed of fibrofatty tissue along with few pilar structures with the focal distribution of granulation tissue. Such a histological picture was found to be consistent with a diagnosis of EAKH.
DISCUSSION
EAKH was proposed as a distinct new entity in 2006 by Kanitakis et al. [1] when they discovered that a case clinically diagnosed as EAH had histology with features of both SAK and EAH and hence they came up with the new terminology. Interestingly, in all the described cases the lesion was present over the right lower limb. In our case, the lesion was present as a small nodular lesion since birth and was soon noticed due to ulceration. Its progression was relatively rapid. The lesions described by other authors presented in late 20s. Ours’ is first case report in the age group of 1.5 years. At the time of presentation, the lesion measured about 4 × 3 cm2, 3 × 2 cm2 and 1 × 1 cm2 (larger than the rest of the cases) and was painless like the other ones. Neither of the patients, in any case, had a significant family history nor anyone had any associated systemic illness/chronic pathology.
EAH is a relatively rare condition that usually manifests at birth (in 50% cases) or early in childhood (~25%) as a papule or a nodule or a plaque on distal portions of the extremities (~80%) [4–7], but they have been reported on other sites including head and neck region and trunk [8, 9]. It commonly presents as a solitary lesion, but the occurrence of multiple EAH has been documented [10–12]. The lesion is usually asymptomatic but may be associated with pain and hyperhidrosis [13]. Most cases of EAH enlarge with body size and sudden enlargement has been noted at puberty and during pregnancy in some probably due to some hormonal correlation. Histologically the lesion affects mainly mid and deep dermis and is composed of lobules of proliferating capillaries intricately admixed with sweat glands and ducts, fat and myxoid tissue.
SAK is a relative commoner condition first described by Imperial and Helwig [2]. They are the most common form of angiokeratomas, and the reported frequency varies from 70 to 83% of all angiokeratomas [14]. SAK tends to affect lower extremities young adults commonly, however, the variety of sites have been documented including the oral cavity. They are seen clinically as a warty, keratotic, red-blue to black papule or nodule and histology is characterized by the presence of thin ectactic capillary vessels in papillary dermis with overlaying epidermis showing verrucous hyperplasia.
Since its recognition, only three cases of EAKH have been documented. Our case is only the fourth in the row and is unique in many aspects.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}