





Abstract
Strangulation of the gallbladder associated with the omentum is extremely rare and, to our knowledge, only two cases have been previously reported. The patient was a 91-year-old female who presented to our emergency room with a chief complaint of upper abdominal pain. Computed tomography imaging revealed a gourd-shaped gallbladder with biphasic appearance divided clearly at the body. In the fundus side, the wall of the gallbladder was oedematous and thickened, while the neck side was intact. On the second day after onset, a laparoscopic cholecystectomy was performed. A tip of the omentum encircling the gallbladder was adhered to the abdominal wall and was strangling the gallbladder. By cutting the omentum at the attachment site, the strangulation was released. Laparoscopic cholecystectomy was performed, and the patient was discharged with an uneventful course. We experienced an extremely rare case of strangulated gallbladder caused by a tip of the omentum attached to the abdominal wall.
INTRODUCTION
Torsion of the gallbladder is a rare clinical condition, and previously, hundreds of cases were reported [1]. On the other hand, strangulation of the gallbladder caused by other conditions is extremely rare, and only several cases were previously reported in the English literature [2–8]. Of these, only two cases were associated with the omentum [2, 3] (Table 1). Here, we report an extremely rare case of a strangulated gallbladder caused by a tip of the omentum.
Clinical characteristics of the patients with strangulated gallbladder associated with omentum previously reported
| Case | Author | Year | Gender | Age | Previous history of surgery | Preoperative diagnosis | Cause of strangulation | Preoperative recurrence of symptoms | Operation |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Ueo | 2006 | Female | 35 | NA | Torsion | A tip of lesser omentum | Present | LC |
| 2 | Miyakura | 2012 | Female | 61 | None | Volvulus | A tip of lesser omentum | Absent | LC |
| 3 | Our case | 2017 | Female | 91 | None | Torsion | A tip of omentum attached to the abdominal wall | Absent | LC |
NA, not announced; LC, laparoscopic cholecystectomy.
※Recurrence was occurred in intra-abdominal lymph nodes and liver 4 months after operation.
CASE REPORT
The patient was a 91-year-old female who presented to our emergency department with the complaint of upper abdominal pain. A physical examination revealed tenderness in the right upper abdomen without signs of peritoneal irritation. She had a previous history of hypertension and was positive for hepatitis C. There was no previous surgical illness. Her body mass index was 21.4 kg/m2. Laboratory data did not show specific abnormal data, including white blood cell count (WBC 4200/μl) and C-reactive protein (CRP 0.01 mg/dl).
A computed tomography (CT) image revealed a gourd-shaped gallbladder with biphasic appearance divided clearly at the body. In the fundus side, the wall of the gallbladder was oedematous and thickened, while the neck side was intact (Fig. 1). The preoperative diagnosis was torsion of the gallbladder. After admission, her abdominal symptoms showed improvement, although they did not disappear completely. On the second day after onset, we planned to perform a laparoscopic cholecystectomy (LC). During laparoscopy, a tip of the omentum encircling the gallbladder was strangling the gallbladder and had adhered to the abdominal wall. By cutting the attachment site of the omentum, the strangulation was released and a whole image of the gallbladder appeared (Fig. 2). The gallbladder was found to have been strangulated by a tip of the omentum attached to the abdominal wall without torsion. The gallbladder was oedematous and congested, although it did not show apparent gangrenous change. We performed LC. The borderline between ischaemic change and non-ischaemic change in the specimen was apparent (Fig. 3).
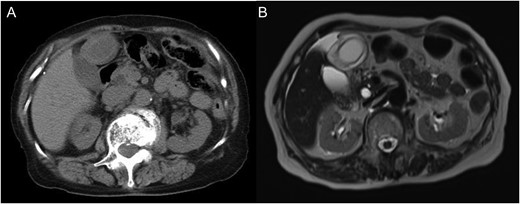
(A) Unenhanced computed tomography image. A gourd-shaped gallbladder with biphasic appearance was revealed. In the fundus side, the wall of the gallbladder appears oedematous and thickened, while the neck side appears intact. (B) T2-weighted magnetic resonance image.
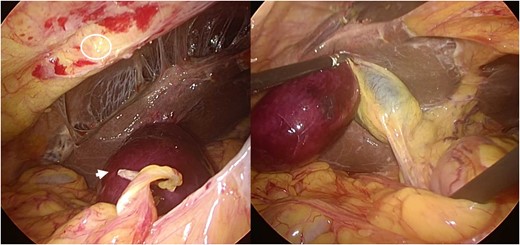
Intraoperative laparoscopic finding. A tip of the omentum encircling the gallbladder adhered to the abdominal wall and strangled the gallbladder. By cutting the attachment site of the omentum, the strangulation was released and a whole image of gallbladder appeared. The gallbladder was found to have been strangulated by the band between the omentum and abdominal wall. A circle shows the attachment site of the omentum at the abdomen. The arrow shows the tips of the omentum, which encircled and strangled the gallbladder.

Resected specimen. A borderline between ischaemic change and non-ischaemic change in the specimen was apparent.
DISCUSSION
In this report, we present an extremely rare case of strangulated gallbladder caused by a tip of the omentum attached to the abdominal wall. Strangulation of the gallbladder may be caused by several kinds of clinical conditions. Of these, torsion or volvulus of the gallbladder may be the most common cause of strangulation [1, 9]. According to previous reports, other conditions causing strangulation include herniation into the foramen Winslow [4–6], incisional hernia [7, 8] and strangulation associated with the omentum [2, 3].
In the present case, preoperative diagnosis was torsion of the gallbladder. Previous reports also preoperatively diagnosed strangulated gallbladder associated with the omentum as a torsion or volvulus of the gallbladder [2, 3]. The radiological findings of torsion of the gallbladder and strangulation associated with the omentum are similar in their biphasic appearance. Hence, it seems difficult to preoperatively distinguish these clinical conditions. However, in cases of torsion of the gallbladder, a V-shaped distortion of the extrahepatic duct or twisting of the cystic artery are often found on the CT image [1.9], which would not be found in the cases with strangulated gallbladder associated with the omentum.
Regarding treatment, surgical resection is the radical treatment for strangulated gallbladder, including those associated with the omentum. LC had also been performed in both of the previous two cases. In the cases of strangulated gallbladder, including those associated with the omentum, compromised blood supply and obstructed biliary drainage will occur [9]. Therefore, the operation should be performed immediately in order to prevent gangrenous change or perforation, which may cause death [9]. On the other hand, in the present case, abdominal symptoms and general conditions of the patient showed a tendency towards improvement, and surgery was performed on the second day after the onset of symptoms. In addition, intraoperative findings in our case showed a gallbladder with a congested appearance without a gangrenous change in the fundus side. The findings from these cases suggested that in cases preoperatively suspected as strangulation of the gallbladder, early operation could be a feasible method instead of immediate operation, if the symptoms and conditions of the patient showed a tendency towards improvement. A case reported by Ueo et al. [2] showed repeated episodes of abdominal pain. This case also suggested the possibility of early operation, before the strangulation developed completely.
In conclusion, we experienced an extremely rare case of strangulated gallbladder caused by the omentum being attached to the abdominal wall. To our knowledge, this was the third case reported in the English literature of strangulated gallbladder associated with the omentum.
CONSENT
The patient discussed in this case report provided her informed consent for publishing the information in this report.
FUNDING
No authors have direct or indirect commercial and financial incentives associated with publishing the article.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.

{kind=link}
{kind=link}
{kind=link}