





Abstract
Massive hemoperitoneum from spontaneous bleeding of uterine myoma is an extremely rare condition, that needs urgent surgical exploration. We report a 40-year-old woman, admitted for acute onset of abdominal pain. Physical examination revealed hypovolemic shock. The hemoglobin level was of 5 g/dL. Ultrasonography revealed hemoperitoneum. Emergency surgical exploration was planned. There was hemoperitoneum of 3 L, uterine myomas with multiple subserous myomas, bleeding from superficial ruptured varice overlying the most largest subserous myoma, which measured 15 cm. Glove adapted as a tourniquet, was applied at the base of the uterus, and myomectomies were performed with removal of around twenty myomas. The postoperative course was uneventful. Myomectomies can be safely and effectively performed by using a tourniquet, for massive hemoperitoneum with precarious hemodynamic status due to subserous myoma bleeding, despite the number and the size of myomas.
INTRODUCTION
Hemoperitoneum is an extremely rare complication of subserous uterine myomas [1]. It is life-threatening condition, due to hemodynamical instability that occured, and needs prompt urgent bloodless exploratory surgery, with procedures varying from myomectomy to hysterectomy, to obtain complete hemostasis and stabilize the patient [2, 3].
Recently, we experienced a nulliparous patient who underwent myomectomies for massive hemoperitoneum with precarious hemodynamic status, from uterine myoma bleeding. This case report presents a rare case of massive hemoperitoneum from spontaneous uterine myoma bleeding managed by myomectomies. To our knowledge, such a case of management by myomectomies for massive hemoperitoneum with precarious hemodynamic status, has not been reported previously.
CASE REPORT
A 40-year-old nulliparous woman, with clinical history of not explored heavy menstrual bleeding, was admitted to the emergency for acute onset of abdominal pain. She did not experience fever, digestive or urinary symptoms.
Physical examination revealed signs of hypovolemic shock, abdominal tenderness with dullness in the flancks.
The patient’s hemoglobin was 5 g/dL. The platelet count, liver et renal function tests were normal. The sensitive urine β-human chorionic gonadotropin test was negative.
Transabdominal ultrasonography revealed a hyperechoic fluid filling almost the entire abdominal cavity, and a huge solid pelvic mass. Regular ovaries were not identified, owing to the pelvic mass size. Abdominal computed tomography was not performed. A diagnosis of intra-abdominal hemorrhage was made. Resuscitation was started immediately with saline solutions perfusion and four units of packed red cells transfusion. The patient was hemodynamically stable, after 30 min, without a need of vasoactive drugs.
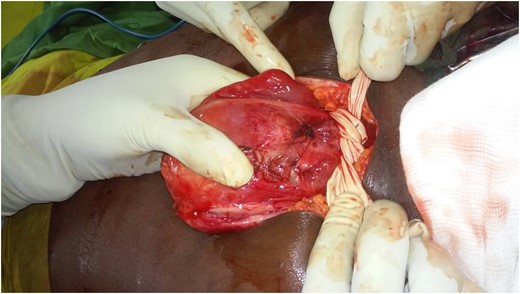
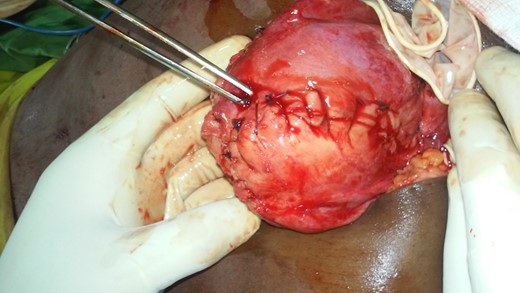
Emergency laparoscopic exploration was planned. Intraoperatively, there was hemoperitoneum of 3 L, large size of uterine myomas with multiple subserous myomas (Fig. 1), hindering abdominal cavity exploration. The laparoscopy was converted to mediane laparotomy. On reaching the abdominal cavity, there was active bleeding from superficial ruptured varice overlying the most largest subserous myoma on the anterior wall of the uterus (Fig. 2), which measured ~15 cm in maximum diameter. The fallopian tubes and ovaries were normal. Other abdominal organs were essentially normal. Sterile glove was adapted as a uterine tourniquet and applied as low as possible at the base of the uterus (Fig. 3), and myomectomies were carried out with removal of around twenty myomas, measuring from 1 to 15 cm, followed by uterine reconstruction. Complete hemostasis has been achieved after the glove removal (Fig. 4).

Posterior wall of uterine myomas showing multiples subserous myomas.

Active bleeding of superficial ruptured varice overlying a subserous myoma.
Glove applied at the base of the uterus.
Uterus after glove removal.
The postoperative course was uneventful. Pathological examination of the resected specimens (Fig. 5) confirmed benign leiomyoma.

Specimen of excised uterine myomas.
DISCUSSION
Myomas are the most common benign neoplasm of the reproductive organs in women of childbearing age [4]. Well-known acute complications of myomas include torsion of a subserosal pedunculated myoma, urinary retention, venous thromboembolism and hemorrhage due to degeneration of a myoma [5]. A large hemorrhage as a result of spontaneous rupture of a vessel overlying a myoma is a rare complication [6].
Imaging modalities, including ultrasound and computed tomography are helpful to make a diagnosis of hemoperitoneum, to quantify it and to identify active bleeding with extravasation of contrast material. They are also helpful to make the differential diagnosis. However, as demonstrated in our case, imaging is unable to pinpoint the source of bleeding [7]. Making an exact diagnosis is often delayed until surgery is performed [3]. Computed tomography was not performed because of the patient precarious hemodynamic status.
The treatment of hemoperitoneum secondary to subserous uterine myoma bleeding depends on the age and parity of the patient, the myoma number, and the bleeding severity. The primary goal should be complete hemostasis. There are different treatment options for patients presenting with subserous uterine myoma bleeding. These treatment options vary from uterine-preserving surgery-myomectomy- to hysterectomy [2, 3].
The absence of prior written patient consent for performing a hysterectomy, the patient’s nulliparity and her intraoperative hemodynamic stability without a need for vasoactives drugs, had prompted us to perform uterine-preserving surgery.
Myomectomy is a surgical procedure associated with heavy bleeding [8]. Enucleating all the numerous myomas of our patient’s uterus, would have certainly led to the occurrence of her precarious hemodynamic compromise, that could be fatal.
Sterile glove applied at the base of the uterus—mechanical tourniquet—has exerted a pressure on uterine arteries, and has minimized intraoperative bleeding [9]. It has permitted an almost bloodless myomectomies, with little intraoperative blood loss, despite the number and the size of the myomas removed, avoiding the occurrence of hemodynamic compromise. The sterile glove form of tourniquet is cheap, safe and effectively reduces blood loss during myomectomies. However, it may mask inadequate hemostasis that only becomes apparent once the tourniquet is removed [8].
In summary, the occurrence of sudden abdominal pain with hypovolemic shock, and signs of peritonism, in a woman of childbearing age, should continue to guide drilling of gynecological aetiologies as the first diagnostic option. However, subserous myoma bleeding should be borne in mind in the differential diagnosis of this condition, especially in nulliparous patients with clinical history suggestive of uterine myoma. This condition needs prompt emergency surgery to stabilize the patient. Myomectomies can be safely and effectively performed even for massive hemoperitoneum with precarious hemodynamic status due to subserous myoma bleeding, by using a mechanical tourniquet.
WRITTEN PATIENT CONSENT
Is available.
CONFLICT OF INTEREST STATEMENT
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}