





Abstract
Post-traumatic pulmonary hernia can occur immediately after thoracic trauma or it may also appear months or even years after the onset. We report a case of a seventeen year-old male patient with thoracic blunt trauma secondary to high energy bicycle accident. Chest CT shows moderate hemothorax and pneumothorax, displaced fracture of the fifth left rib, and protusion of pulmonary tissue through a chest wall defect. In the Emergency Room the patient presents with chest pain (7/10 in Visual Analog Scale) and respiratory distress. Video-assisted thoracic surgery approach was chosen. Hernia reduction, non-anatomic lingular resection and rib fracture external fixation using a titanium plate was performed. Traumatic pulmonary hernia is an uncommon complication of thoracic trauma which may constitute an emergency for the trauma or thoracic surgeon. The early management of this injury can be developed by minimally invasive approach with excellent results.
INTRODUCTION
Lung herniation is defined as the protrusion of the lung through an abnormal opening in the chest wall. In 1847, Morel-Lavallée [1] classified lung herniation into cervical, thoracic or diaphragmatic. Lung herniation can also be classified based on congenital or acquired etiology (traumatic, spontaneous or pathological cause).
Since Roland’s first case report in 1499 [2], ~300 cases have been reported in the international literature. Overall, 85% of lung herniation is caused by trauma (65% thoracic, 35% cervical and <1% diaphragmatic) [3]. There are also spontaneous cases reported, which are mainly caused by valsalva maneuver [4] and pathological cases caused by infectious diseases such as tuberculosis [5].
Chest trauma may be caused by penetrating or blunt mechanisms. Blunt trauma is however more frequent in occurrence. If lung herniation has occurred, chest pain, dyspnea, subcutaneous emphysema, bone crepitation and hemoptysis (in case of damage of the lung parenchyma) may be present.
In the absence of higher quality evidence, most knowledge of this pathology comes from case reports.
Conservative management has been described in both adults and children [6], but most case reports describe surgical management [7–9].
Besides surgical indications, there is controversy regarding intraoperative decisions such as lung resection, rib fixation and chest wall reconstruction with prosthetic material.
To our knowledge, this is the first reported case of surgical management in lung herniation and rib fracture fixation with prosthetic material through a minimally invasive approach.
CASE REPORT
A 17-year-old man with no past medical history had a downhill bicycling accident. He lost control of his bicycle and crashed against a retaining wall of the road. He was taken to the Emergency Department where he presented with chest pain and shortness of breath.
On physical examination he had mild tachycardia and tachypnea. His vital signs were as follows: BP: 123/83 mmHg, HR: 105 bpm, SO2 95% (FiO2 21%) and RR: 25 bpm. On thoracic examination, he had decreased breath sounds in the lower portion of the chest, pain and bone crepitation over the fifth rib.
The chest CT showed moderate hemothorax, pneumothorax, a displaced fracture of the fifth left rib, and protrusion of a lung segment through a chest wall defect (Fig. 1).
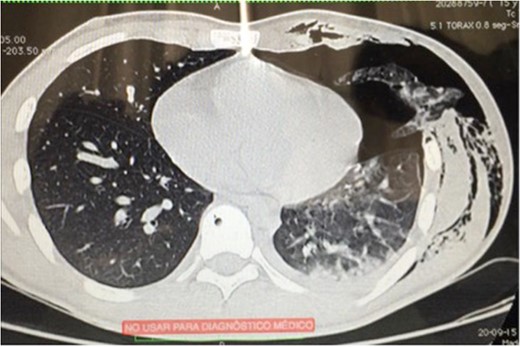
Chest CT scan showing pneumothorax and lung herniation.
A chest tube was inserted through the fourth left intercostal space (ICS) and connected to a water seal device (Aquaseal TM) on −20 cm H2O suction.
Video-assisted thoracic surgery (VATS) was indicated. The port placements were inserted as following: Port 1 into the seventh ICS on the anterior axillary line. Port 2 into the fifth ICS on the posterior axillary line. Port 3 into the second ICS on the anterior axillary line.
A lingular lung segment protruding through the fifth ICS was observed (Fig. 2), as well as a moderate hemothorax. Lung tissue reduction was performed.
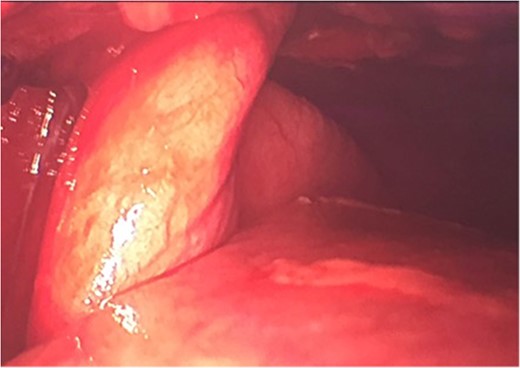
Lung herniation seen through VATS pleuroscopy.
Due to the macroscopic appearance of ischemia and venous congestion of the involved lung tissue, a non-anatomic lingular resection using 60 mm Echelon Flex Stappler® was performed (Fig. 3) as well as a chest washout.

Wedge resection of ischemic lung through chest wall herniation.
A longitudinal incision was made over the fractured rib (Fig. 4). A displaced rib fracture was observed. Bone segments were reduced and fixed using a 6 cm titanium plate (STRATOSTM System). A chest tube was inserted through the seventh ICS and connected to a closed water seal device on suction (Fig. 5).

Reduced rib fracture previous to rib fixation.
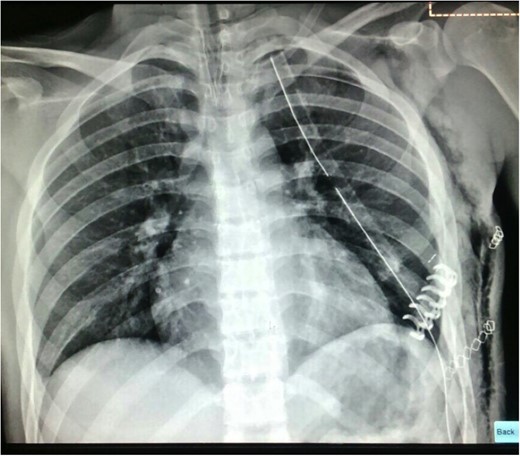
Post-operative chest X ray in recovery room.
The patient had significant relief of his symptoms. The chest tube was removed and the patient was discharged on the second post-operative day with minimal requirements for analgesics (oral paracetamol).
DISCUSSION
Due to its rarity and high variability of presentation, there is insufficient evidence in the literature to recommend a standard management of the traumatic lung herniation.
Based on this case and the review of the literature, we would like to make the following recommendations for the management of similar cases:
Surgical approach
The approach will depend on the number of injured rib segments and the anterior or posterior rib location. We recommend performing a video-assisted exploration first, which aids in the subsequent surgical decision making.
Exhaustive exploration for other intrathoracic injuries
Start looking for causes of active bleeding, such as great vessels, subclavian vessels, azygos system or intercostal vessels injuries. It is important to look for lung or diaphragmatic injuries that can be easily repaired in the same surgery.
Critical evaluation of the herniated lung segment
The herniated lung tissue vitality may be compromised. If there are doubts about the vitality of the affected tissue, we recommend performing a non-anatomic resection of the involved segment.
Rib fracture fixation
There is insufficient evidence to recommend external fixation in all the cases. In this case, we elected to perform an external fixation of the fracture with prosthetic material due to the instability of the fracture and the risk of shear with the respiratory movements.
Chest wall reconstruction
It may be sufficient to perform primary muscle closure with absorbable suture material. However, in cases of considerable chest wall disruption, it may be necessary to perform a chest wall reconstruction using a muscle flap or mesh.
Decisions in the management of lung herniation must be done on a case-by-case basis.
FUNDING
There was no financial support in the realization of this case report.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}